
Effects of Gluten on Gut Microbiota in Patients with Gastrointestinal Disorders, Migraine, and Dermatitis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Biomarker Analysis
2.4. MIDAS Questionnaire
2.5. Molecular Analysis
2.5.1. DNA Extraction
2.5.2. DNA Quality
2.5.3. Library Construction
2.5.4. Next-Generation Sequencing
2.6. Bioinformatics Analysis
2.7. Statistical Analysis
2.8. Ethical Considerations
3. Results
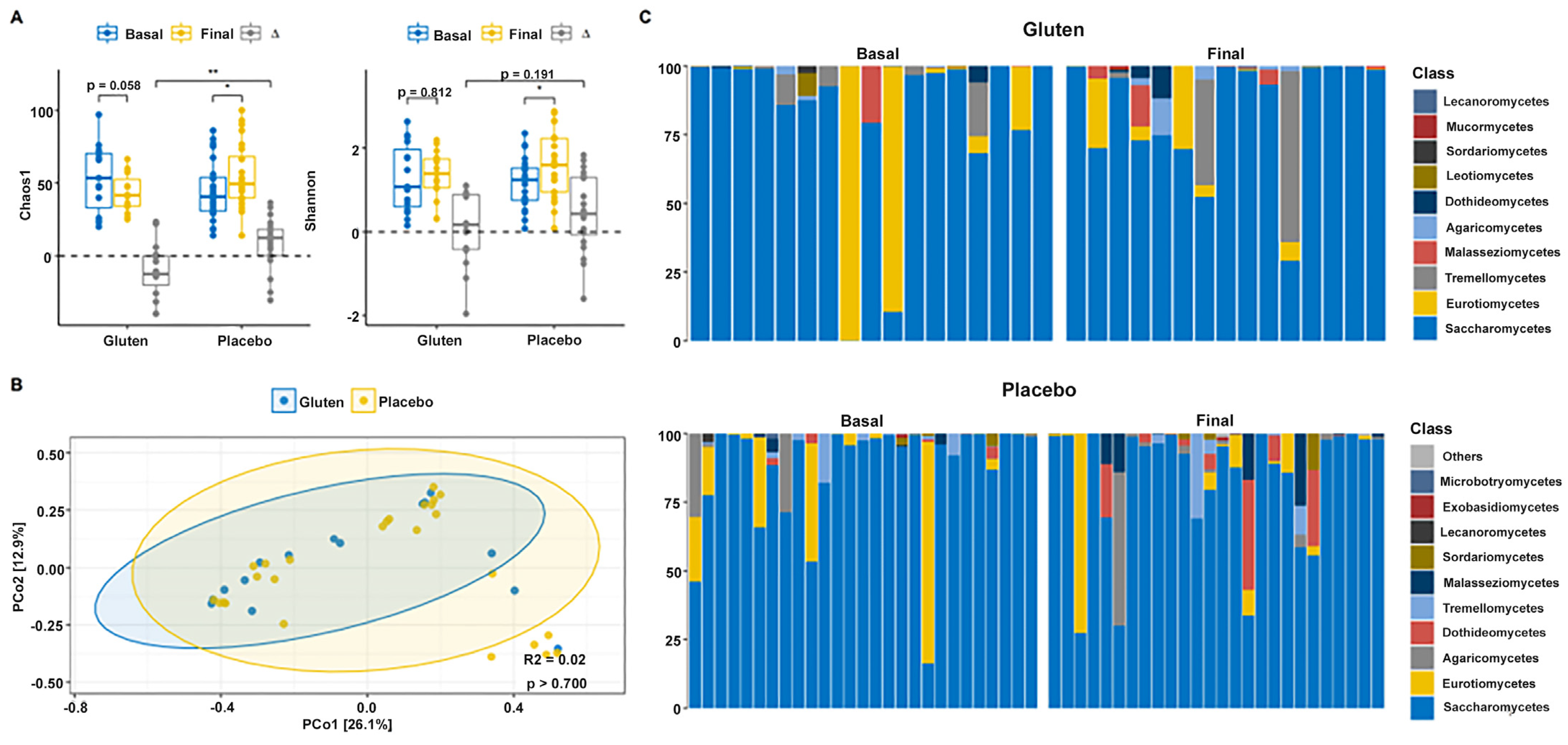
3.1. Diversity and Fungal Composition
3.2. Bacterial Diversity and Composition
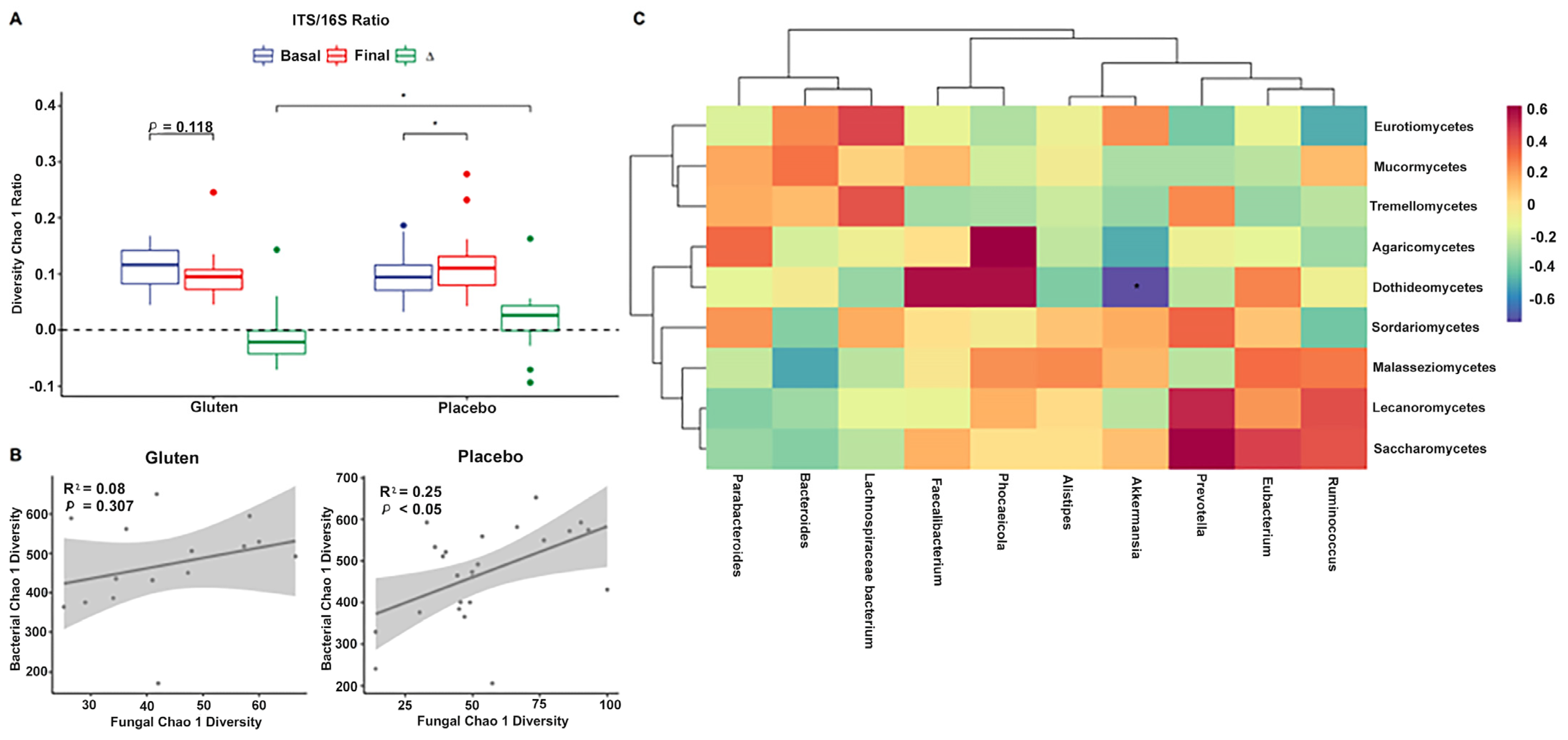
3.3. Relationship between ITS and 16S rRNA Gene Amplicon Sequencing Data
3.4. GI Disorders, Migraine, and Atopic Dermatitis
3.5. Biomarkers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Böhn, L.; Störsrud, S.; Törnblom, H.; Bengtsson, U.; Simrén, M. Self-reported food-related gastrointestinal symptoms in IBS are common and associated with more severe symptoms and reduced quality of life. Am. J. Gastroenterol. 2013, 108, 634–641. [Google Scholar] [CrossRef] [PubMed]
- Barbaro, M.R.; Cremon, C.; Wrona, D.; Fuschi, D.; Marasco, G.; Stanghellini, V.; Barbara, G. Non-Celiac Gluten Sensitivity in the Context of Functional Gastrointestinal Disorders. Nutrients 2020, 12, 3735. [Google Scholar] [CrossRef] [PubMed]
- Aziz, I. The Global Phenomenon of Self-Reported Wheat Sensitivity. Am. J. Gastroenterol. 2018, 113, 945–948. [Google Scholar] [CrossRef] [PubMed]
- Dieterich, W.; Schuppan, D.; Schink, M.; Schwappacher, R.; Wirtz, S.; Agaimy, A.; Neurath, M.F.; Zopf, Y. Influence of low FODMAP and gluten-free diets on disease activity and intestinal microbiota in patients with non-celiac gluten sensitivity. Clin. Nutr. 2019, 38, 697–707. [Google Scholar] [CrossRef] [PubMed]
- Zanini, B.; Baschè, R.; Ferraresi, A.; Ricci, C.; Lanzarotto, F.; Marullo, M.; Villanacci, V.; Hidalgo, A.; Lanzini, A. Randomised clinical study: Gluten challenge induces symptom recurrence in only a minority of patients who meet clinical criteria for non-coeliac gluten sensitivity. Aliment. Pharmacol. Ther. 2015, 42, 968–976. [Google Scholar] [CrossRef] [PubMed]
- Biesiekierski, J.R.; Peters, S.L.; Newnham, E.D.; Rosella, O.; Muir, J.G.; Gibson, P.R. No effects of gluten in patients with self-reported non-celiac gluten sensitivity after dietary reduction of fermentable, poorly absorbed, short-chain carbohydrates. Gastroenterology 2013, 145, 320–328.e83. [Google Scholar] [CrossRef]
- Junker, Y.; Zeissig, S.; Kim, S.J.; Barisani, D.; Wieser, H.; Leffler, D.A.; Zevallos, V.; Libermann, T.A.; Dillon, S.; Freitag, T.L.; et al. Wheat amylase trypsin inhibitors drive intestinal inflammation via activation of toll-like receptor 4. J. Exp. Med. 2012, 209, 2395–2408. [Google Scholar] [CrossRef] [PubMed]
- Zevallos, V.F.; Raker, V.; Tenzer, S.; Jimenez-Calvente, C.; Ashfaq-Khan, M.; Rüssel, N.; Pickert, G.; Schild, H.; Steinbrink, K.; Schuppan, D. Nutritional Wheat Amylase-Trypsin Inhibitors Promote Intestinal Inflammation via Activation of Myeloid Cells. Gastroenterology 2017, 152, 1100–1113.e12. [Google Scholar] [CrossRef]
- Karakula-Juchnowicz, H.; Rog, J.; Juchnowicz, D.; Łoniewski, I.; Skonieczna-Żydecka, K.; Krukow, P.; Futyma-Jedrzejewska, M.; Kaczmarczyk, M. The study evaluating the effect of probiotic supplementation on the mental status, inflammation, and intestinal barrier in major depressive disorder patients using gluten-free or gluten-containing diet (SANGUT study): A 12-week, randomized, double-blind, and placebo-controlled clinical study protocol. Nutr. J. 2019, 18, 50. [Google Scholar] [CrossRef]
- Daulatzai, M.A. Non-celiac gluten sensitivity triggers gut dysbiosis, neuroinflammation, gut-brain axis dysfunction, and vulnerability for dementia. CNS Neurol. Disord. Drug Targets 2015, 14, 110–131. [Google Scholar] [CrossRef]
- Cámara-Lemarroy, C.R.; Rodriguez-Gutierrez, R.; Monreal-Robles, R.; Marfil-Rivera, A. Gastrointestinal disorders associated with migraine: A comprehensive review. World J. Gastroenterol. 2016, 22, 8149–8160. [Google Scholar] [CrossRef]
- Zis, P.; Julian, T.; Hadjivassiliou, M. Headache Associated with Coeliac Disease: A Systematic Review and Meta-Analysis. Nutrients 2018, 10, 1445. [Google Scholar] [CrossRef]
- Hadjivassiliou, M.; Grünewald, R.A.; Lawden, M.; Davies-Jones, G.A.; Powell, T.; Smith, C.M. Headache and CNS white matter abnormalities associated with gluten sensitivity. Neurology 2001, 56, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Collin, P.; Salmi, T.T.; Hervonen, K.; Kaukinen, K.; Reunala, T. Dermatitis herpetiformis: A cutaneous manifestation of coeliac disease. Ann. Med. 2017, 49, 23–31. [Google Scholar] [CrossRef]
- Nosrati, A.; Afifi, L.; Danesh, M.J.; Lee, K.; Yan, D.; Beroukhim, K.; Ahn, R.; Liao, W. Dietary modifications in atopic dermatitis: Patient-reported outcomes. J. Dermatol. Treat. 2017, 28, 523–538. [Google Scholar] [CrossRef]
- Forbes, J.D.; Van Domselaar, G.; Bernstein, C.N. The Gut Microbiota in Immune-Mediated Inflammatory Diseases. Front. Microbiol. 2016, 7, 1081. [Google Scholar] [CrossRef] [PubMed]
- Shreiner, A.B.; Kao, J.Y.; Young, V.B. The gut microbiome in health and in disease. Curr. Opin. Gastroenterol. 2015, 31, 69–75. [Google Scholar] [CrossRef]
- Caio, G.; Lungaro, L.; Segata, N.; Guarino, M.; Zoli, G.; Volta, U.; De Giorgio, R. Effect of Gluten-Free Diet on Gut Microbiota Composition in Patients with Celiac Disease and Non-Celiac Gluten/Wheat Sensitivity. Nutrients 2020, 12, 1832. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Elli, L.; Bonaz, B.; Bouma, G.; Carroccio, A.; Castillejo, G.; Cellier, C.; Cristofori, F.; de Magistris, L.; Dolinseket, J.; et al. Diagnosis of Non-Celiac Gluten Sensitivity (NCGS): The Salerno Experts’ Criteria. Nutrients 2015, 7, 4966–4977. [Google Scholar] [CrossRef]
- Fasano, A. Zonulin and its regulation of intestinal barrier function: The biological door to inflammation, autoimmunity, and cancer. Physiol. Rev. 2011, 91, 151–175. [Google Scholar] [CrossRef]
- Fasano, A. Zonulin, regulation of tight junctions, and autoimmune diseases. Ann. N. Y Acad. Sci. 2012, 1258, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Stewart, W.F.; Lipton, R.B.; Kolodner, K.; Liberman, J.; Sawyer, J. Reliability of the migraine disability assessment score in a population-based sample of headache sufferers. Cephalalgia 1999, 19, 107–174. [Google Scholar] [CrossRef] [PubMed]
- Edgar, R.C. Search and clustering orders of magnitude faster than BLAST. Bioinformatics 2010, 26, 2460–2461. [Google Scholar] [CrossRef] [PubMed]
- Liu, C.; Cui, Y.; Li, X.; Yao, M. microeco: An R package for data mining in microbial community ecology. FEMS Microbiol. Ecol. 2021, 97, fiaa255. [Google Scholar] [CrossRef] [PubMed]
- Mallick, H.; Rahnavard, A.; McIver, L.J.; Ma, S.; Zhang, Y.; Nguyen, L.H.; Tickle, T.L.; Weingart, G.; Ren, B.; Schwager, E.H.; et al. Multivariable association discovery in population-scale meta-omics studies. PLoS Comput. Biol. 2021, 17, e1009442. [Google Scholar] [CrossRef]
- Bernardo, D.; Garrote, J.A.; Nadal, I.; León, A.J.; Calvo, C.; Fernández-Salazar, L.; Blanco-Quirós, A.; Sanz, Y.; Arranz, E. Is it true that coeliacs do not digest gliadin? Degradation pattern of gliadin in coeliac disease small intestinal mucosa. Gut 2009, 58, 886–887. [Google Scholar] [CrossRef] [PubMed]
- Ponzo, V.; Ferrocino, I.; Goitre, I.; Pellegrini, M.; Bruno, M.; Astegiano, M.; Cadario, G.; Castellana, E.; Bioletto, F.; Corvaglia, M.R.; et al. Non-Celiac Gluten/Wheat Sensitivity: Clinical Characteristics and Microbiota and Mycobiota Composition by Response to the Gluten Challenge Test. Nutrients 2021, 13, 1260. [Google Scholar] [CrossRef] [PubMed]
- Caminero, A.; Herrán, A.R.; Nistal, E.; Pérez-Andrés, J.; Vaquero, L.; Vivas, S.; Ruiz de Morales, J.M.; Albillos, S.M.; Casqueiro, J. Diversity of the cultivable human gut microbiome involved in gluten metabolism: Isolation of microorganisms with potential interest for coeliac disease. FEMS Microbiol. Ecol. 2014, 88, 309–319. [Google Scholar] [CrossRef] [PubMed]
- De Palma, G.; Nadal, I.; Collado, M.C.; Sanz, Y. Effects of a gluten-free diet on gut microbiota and immune function in healthy adult human subjects. Br. J. Nutr. 2009, 102, 1154–1160. [Google Scholar] [CrossRef]
- Nadal, I.; Donant, E.; Ribes-Koninckx, C.; Calabuig, M.; Sanz, Y. Imbalance in the composition of the duodenal microbiota of children with coeliac disease. J. Med. Microbiol. 2008, 57, 401, Erratum in J. Med. Microbiol. 2007, 56, 1669–1674. [Google Scholar] [CrossRef]
- Bascuñán, K.A.; Araya, M.; Roncoroni, L.; Doneda, L.; Elli, L. Dietary Gluten as a Conditioning Factor of the Gut Microbiota in Celiac Disease. Adv. Nutr. 2020, 11, 160–174. [Google Scholar] [CrossRef] [PubMed]
- Tjellström, B.; Högberg, L.; Stenhammar, L.; Fälth-Magnusson, K.; Magnusson, K.E.; Norin, E.; Sundqvist, T.; Midtvedt, T. Faecal short-chain fatty acid pattern in childhood coeliac disease is normalised after more than one year’s gluten-free diet. Microb. Ecol. Health Dis. 2013, 24, 20905. [Google Scholar] [CrossRef] [PubMed]
- Nash, A.K.; Auchtung, T.A.; Wong, M.C.; Smith, D.P.; Gesell, J.R.; Ross, M.C.; Stewart, C.J.; Metcalf, G.A.; Muzny, D.M.; Gibbs, R.A.; et al. The gut mycobiome of the Human Microbiome Project healthy cohort. Microbiome 2017, 5, 153. [Google Scholar] [CrossRef] [PubMed]
- Mukherjee, P.K.; Sendid, B.; Hoarau, G.; Colombel, J.F.; Poulain, D.; Ghannoum, M.A. Mycobiota in gastrointestinal diseases. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 77–87. [Google Scholar] [CrossRef] [PubMed]
- Richard, M.L.; Sokol, H. The gut mycobiota: Insights into analysis, environmental interactions and role in gastrointestinal diseases. Nat. Rev. Gastroenterol. Hepatol. 2019, 16, 331–345. [Google Scholar] [CrossRef] [PubMed]
- Chin, V.K.; Yong, V.C.; Chong, P.P.; Amin Nordin, S.; Basir, R.; Abdullah, M. Mycobiome in the Gut: A Multiperspective Review. Mediat. Inflamm. 2020, 2020, 9560684. [Google Scholar] [CrossRef] [PubMed]
- Mateo, E.M.; Tarazona, A.; Jiménez, M.; Mateo, F. Lactic Acid Bacteria as Potential Agents for Biocontrol of Aflatoxigenic and Ochratoxigenic Fungi. Toxins 2022, 14, 807. [Google Scholar] [CrossRef] [PubMed]
- Zhang, T.; Li, Q.; Cheng, L.; Buch, H.; Zhang, F. Akkermansia muciniphila is a promising probiotic. Microb. Biotechnol. 2019, 12, 1109–1125. [Google Scholar] [CrossRef]
- Röhrig, L.; Dussart, F. Does Abiotic Host Stress Favour Dothideomycete-Induced Disease Development? Plants 2022, 11, 1615. [Google Scholar] [CrossRef]
- Verdu, E.F.; Armstrong, D.; Murray, J.A. Between celiac disease and irritable bowel syndrome: The “no man’s land” of gluten sensitivity. Am. J. Gastroenterol. 2009, 104, 1587–1594. [Google Scholar] [CrossRef]
- Biesiekierski, J.R.; Newnham, E.D.; Irving, P.M.; Barrett, J.S.; Haines, M.; Doecke, J.D.; Shepherd, S.J.; Muir, J.G.; Gibson, P.R. Gluten causes gastrointestinal symptoms in subjects without celiac disease: A double-blind randomized placebo-controlled trial. Am. J. Gastroenterol. 2011, 106, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Dimitrova, A.K.; Ungaro, R.C.; Lebwohl, B.; Lewis, S.K.; Tennyson, C.A.; Green, M.W.; Babyatsky, M.W.; Green, P.H. Prevalence of migraine in patients with celiac disease and inflammatory bowel disease. Headache 2013, 53, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Hervonen, K.; Salmi, T.T.; Ilus, T.; Paasikivi, K.; Vornanen, M.; Laurila, K.; Lindfors, K.; Viiri, K.; Saavalainen, P.; Collin, P.; et al. Dermatitis Herpetiformis Refractory to Gluten-free Dietary Treatment. Acta Derm. Venereol. 2016, 96, 82–86. [Google Scholar] [CrossRef]
- Bardella, M.T.; Fredella, C.; Trovato, C.; Ermacora, E.; Cavalli, R.; Saladino, V.; Prampolini, L. Long-term remission in patients with dermatitis herpetiformis on a normal diet. Br. J. Dermatol. 2003, 149, 968–971. [Google Scholar] [CrossRef] [PubMed]
- Garioch, J.J.; Lewis, H.M.; Sargent, S.A.; Leonard, J.N.; Fry, L. 25 years’ experience of a gluten-free diet in the treatment of dermatitis herpetiformis. Br. J. Dermatol. 1994, 131, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Paek, S.Y.; Steinberg, S.M.; Katz, S.I. Remission in dermatitis herpetiformis: A cohort study. Arch. Dermatol. 2011, 147, 301–305. [Google Scholar] [CrossRef]
- Mansikka, E.; Hervonen, K.; Kaukinen, K.; Ilus, T.; Oksanen, P.; Lindfors, K.; Laurila, K.; Hietikko, M.; Taavela, J.; Jernman, J.; et al. Gluten Challenge Induces Skin and Small Bowel Relapse in Long-Term Gluten-Free Diet-Treated Dermatitis Herpetiformis. J. Investig. Dermatol. 2019, 139, 2108–2114. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gluten Group (n = 17) | Placebo Group (n = 29) | p | |
|---|---|---|---|
| Age (mean ± standard deviation) | 41.59 ± 9.24 | 41.28 ± 8.93 | 0.910 |
| Sex, n (%) | |||
| Women | 11 (64.7) | 25 (86.2) | 0.139 |
| Men | 6 (35.3) | 4 (13.8) | |
| Body mass index, (median (interquartile range)) | 23.8 (21.4–27.8) | 24.6 (22.95–27.05) | 0.482 |
| Gastrointestinal (GI) symptoms, n (%) | |||
| Abdominal pain | 15 (88.2) | 22 (75.9) | 0.450 |
| Bloating | 12 (70.6) | 26 (89.7) | 0.125 |
| Flatulence | 15 (88.2) | 27 (93.1) | 0.619 |
| Diarrhea | 9 (52.9) | 13 (44.8) | 0.761 |
| Stomach sounds | 11 (64.7) | 24 (82.8) | 0.282 |
| Constipation | 6 (35.3) | 11 (37.9) | 1 |
| Urge to defecate | 9 (52.9) | 16 (55.2) | 1 |
| Incomplete evacuation | 9 (52.9) | 21 (72.4) | 0.213 |
| Nausea | 10 (58.8) | 6 (20.7) | 0.012 |
| Burning | 8 (47.1) | 14 (48.3) | 1 |
| Belching | 9 (52.9) | 15 (51.7) | 1 |
| Acid regurgitation | 6 (35.3) | 9 (31) | 1 |
| Epigastric pain | 8 (47.1) | 13 (44.8) | 1 |
| Gluten Group (n = 17) | Placebo Group (n = 27) | ∆Intergroup Analysis | |||||
|---|---|---|---|---|---|---|---|
| GI Disorders | Basal | Final | p | Basal | Final | p | |
| Abdominal pain | 2 (1–2) | 1 (0–1) | 0.013 | 1 (0.5–2) | 0 (0–1) | 0.001 | ns |
| Bloating | 1 (0–2) | 1 (0–1) | 0.033 | 2 (1–3) | 1 (0–2) | 0.000 | ns |
| Flatulence | 1 (1–2) | 1 (0–1) | 0.008 | 2 (2–3) | 1 (0–2) | 0.001 | ns |
| Diarrhea | 1 (0–1) | 0 (0–0) | 0.008 | 0 (0–2) | 0 (0–0) | 0.004 | ns |
| Stomach sounds | 1 (0–2) | 0 (0–1) | 0.031 | 2 (1–2) | 0 (0–1) | 0.000 | ns |
| Reduced consistency | 1 (1–2) | 0 (0–1) | 0.003 | 1 (0–2) | 0 (0–0) | 0.001 | ns |
| Constipation | 0 (0–1) | 1 (0–1) | 0.305 | 0 (0–1.5) | 0 (0–1) | 0.177 | ns |
| Urge to defecate | 1 (0–2) | 0 (0–1) | 0.031 | 1 (0–2.5) | 0 (0–1) | 0.056 | ns |
| Incomplete evacuation | 1 (0–2) | 1 (0–2) | 0.886 | 1 (0.5–2) | 1 (0–1) | 0.033 | ns |
| Nausea | 1 (0–2) | 0 (0–0) | 0.021 | 0 (0–0) | 0 (0–0) | 0.125 | ns |
| Burning | 0 (0–1) | 0 (0–1) | 0.480 | 0 (0–1) | 0 (0–1) | 0.109 | ns |
| Belching | 1 (0–2) | 0 (0–1) | 0.021 | 1 (0–1) | 0 (0–1) | 0.388 | ns |
| Acid regurgitation | 0 (0–1) | 0 (0–0) | 0.375 | 0 (0–0.5) | 0 (0–0.5) | 1 | ns |
| Epigastric pain | 0 (0–2) | 0 (0–0) | 0.068 | 0 (0–1) | 0 (0–0) | 0.017 | ns |
| Depositions | 3.24 ± 2.02 | 2.76 ± 1.79 | 0.290 | 3 (2–6) | 3 (1–4.5) | 0.454 | ns |
| Bristol stool scale | 4.24 ± 1.09 | 3.29 ± 1.53 | 0.016 | 4 (4–5) | 4 (2.5–4) | 0.047 | ns |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
San Mauro Martín, I.; López Oliva, S.; Garicano Vilar, E.; Sánchez Niño, G.M.; Penadés, B.F.; Terrén Lora, A.; Sanz Rojo, S.; Collado Yurrita, L. Effects of Gluten on Gut Microbiota in Patients with Gastrointestinal Disorders, Migraine, and Dermatitis. Nutrients 2024, 16, 1228. https://doi.org/10.3390/nu16081228
San Mauro Martín I, López Oliva S, Garicano Vilar E, Sánchez Niño GM, Penadés BF, Terrén Lora A, Sanz Rojo S, Collado Yurrita L. Effects of Gluten on Gut Microbiota in Patients with Gastrointestinal Disorders, Migraine, and Dermatitis. Nutrients. 2024; 16(8):1228. https://doi.org/10.3390/nu16081228
Chicago/Turabian StyleSan Mauro Martín, Ismael, Sara López Oliva, Elena Garicano Vilar, Guerthy Melissa Sánchez Niño, Bruno F. Penadés, Ana Terrén Lora, Sara Sanz Rojo, and Luis Collado Yurrita. 2024. "Effects of Gluten on Gut Microbiota in Patients with Gastrointestinal Disorders, Migraine, and Dermatitis" Nutrients 16, no. 8: 1228. https://doi.org/10.3390/nu16081228