
The Effect of Post-Graduate Year Training on the Self-Efficacy and Emotional Traits of Physicians Facing the COVID-19 Pandemic


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample Estimation
2.2. Questionnaires for the Study
2.3. Data Processing
2.4. Statistical Analysis
3. Results
3.1. Basic Sociodemographic Characteristics of the Study Population
3.2. Factor Analysis of the Questionnaire
3.3. Measurement of the Self-Efficacy and Emotional Traits of the Participants with Different Seniority Levels
3.4. Comparison of the Self-Efficacy and Emotional Traits of the Participants with or without PGY Training
3.5. Comparison of the Self-Efficacy and Emotional Traits of Participants with or without Experience of Caring for Patients with SARS
3.6. Comparison of the Self-Efficacy and Emotional Traits of the Participants with or without Experience of Caring for Patients with SARS in Their Actual Caring for COVID-19 Patients
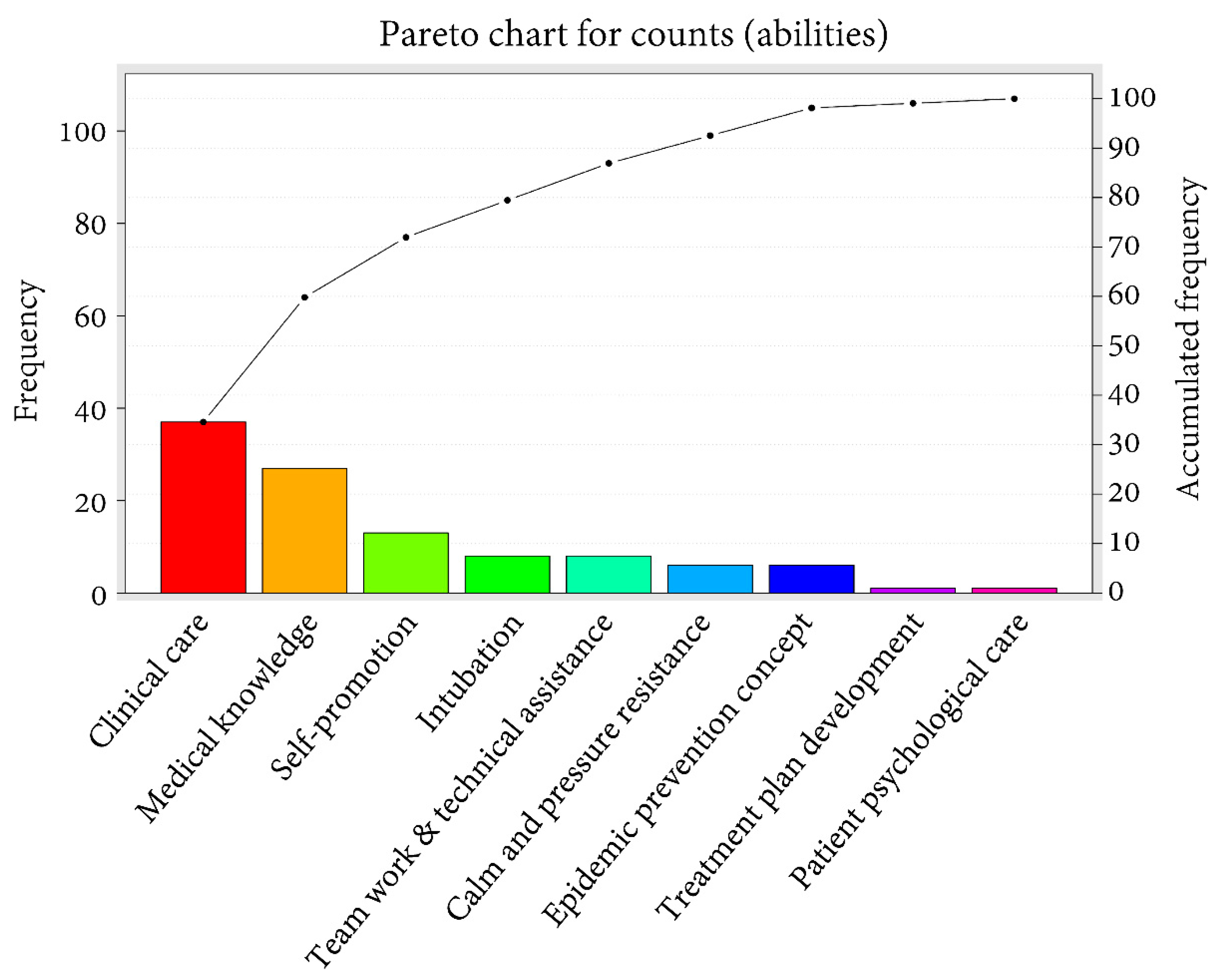
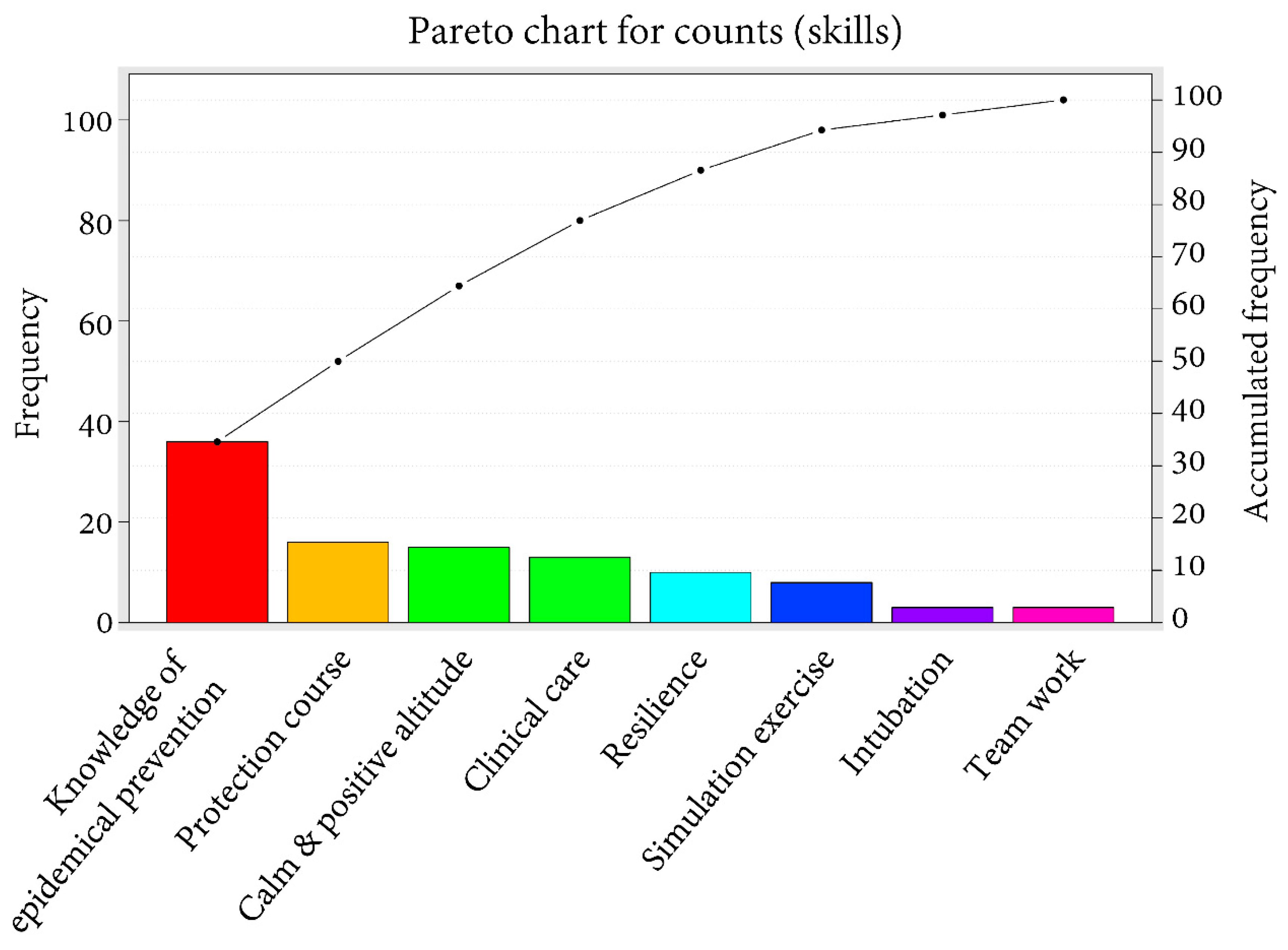
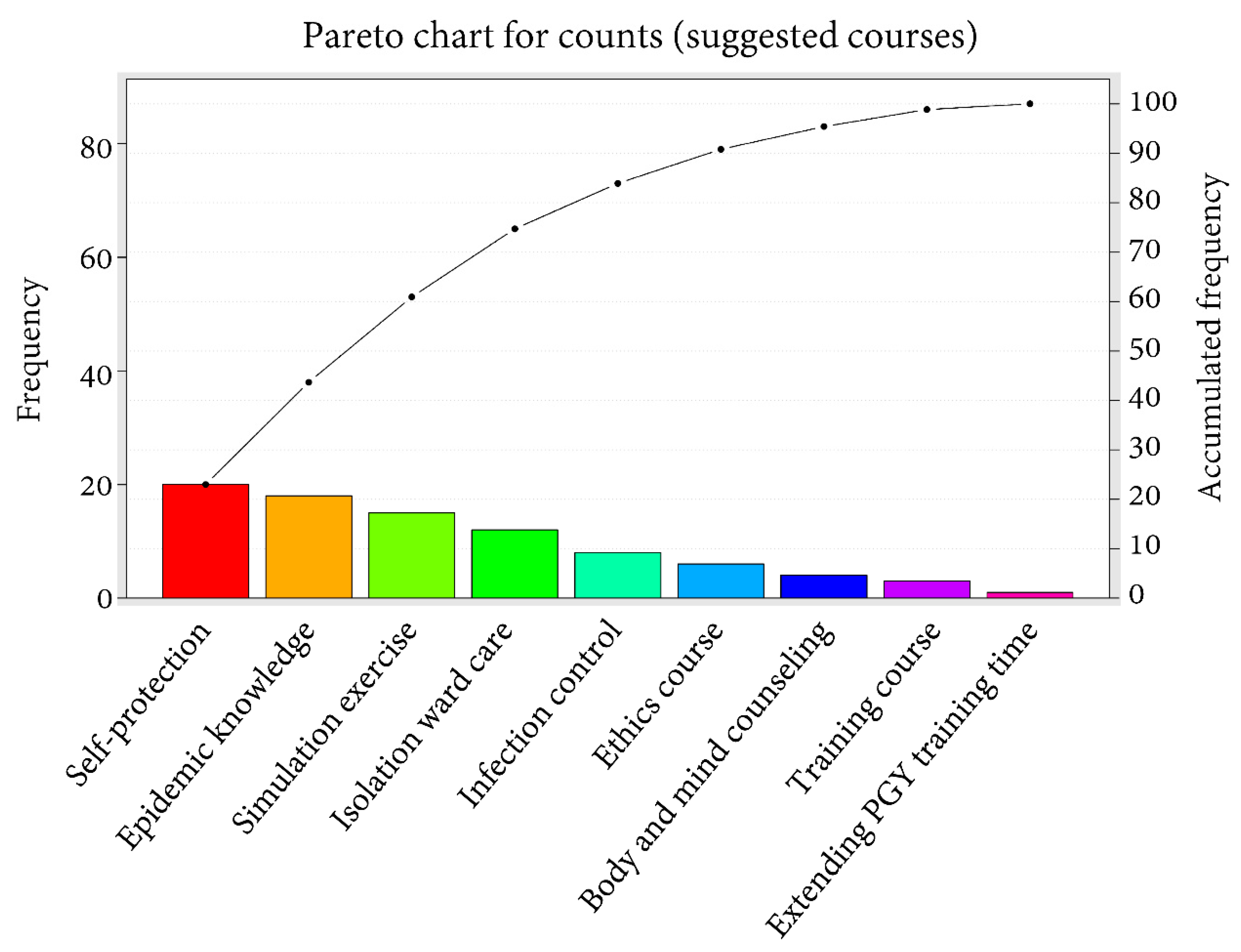
3.7. Feedback and Suggestions Section
4. Discussion
5. Limitations of This Study
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, S.H.; Juang, Y.Y.; Su, Y.J.; Lee, H.L.; Lin, Y.H.; Chao, C.C. Facing SARS: Psychological impacts on SARS team nurses and psychiatric services in a Taiwan general hospital. Gen. Hosp. Psychiatry 2005, 27, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Cassie, J.M.; Armbruster, J.S.; Bowmer, M.I.; Leach, D.C. Accreditation of postgraduate medical education in the United States and Canada: A comparison of two systems. Med. Educ. 1999, 33, 493–498. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.Y.; Lee, F.Y.; Hsu, H.C.; Huang, C.C.; Chen, J.W.; Cheng, H.M.; Lee, W.S.; Chuang, C.L.; Chang, C.C.; Huang, C.C. Assessment of first-year post-graduate residents: Usefulness of multiple tools. J. Chin. Med. Assoc. JCMA 2011, 74, 531–538. [Google Scholar] [CrossRef] [Green Version]
- Chu, T.S.; Weed, H.G.; Wu, C.C.; Hsu, H.Y.; Lin, J.T.; Hsieh, B.S. A programme of accelerated medical education in Taiwan. Med. Teach. 2009, 31, e74. [Google Scholar] [CrossRef] [PubMed]
- Hsu, P.W.; Fu, R.H.; Chang, Y.C. Comparing learning outcomes among postgraduate year trainee groups. Biomed. J. 2020, 43, 490–495. [Google Scholar] [CrossRef]
- Lee, F.Y.; Yang, Y.Y.; Hsu, H.C.; Chuang, C.L.; Lee, W.S.; Chang, C.C.; Huang, C.C.; Chen, J.W.; Cheng, H.M.; Jap, T.S. Clinical instructors’ perception of a faculty development programme promoting postgraduate year-1 (PGY1) residents’ ACGME six core competencies: A 2-year study. BMJ Open 2011, 1, e000200. [Google Scholar] [CrossRef]
- Khan, M.; Adil, S.F.; Alkhathlan, H.Z.; Tahir, M.N.; Saif, S.; Khan, M.; Khan, S.T. COVID-19: A Global Challenge with Old History, Epidemiology and Progress So Far. Molecules 2020, 26, 39. [Google Scholar] [CrossRef]
- Sofi, M.S.; Hamid, A.; Bhat, S.U. SARS-CoV-2: A critical review of its history, pathogenesis, transmission, diagnosis and treatment. Biosaf. Health 2020, 2, 217–225. [Google Scholar] [CrossRef]
- Xie, Y.; Wang, Z.; Liao, H.; Marley, G.; Wu, D.; Tang, W. Epidemiologic, clinical, and laboratory findings of the COVID-19 in the current pandemic: Systematic review and meta-analysis. BMC Infect. Dis. 2020, 20, 640. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, S.; Baticulon, R.E.; Kadhum, M.; Alser, M.; Ojuka, D.K.; Badereddin, Y.; Kamath, A.; Parepalli, S.A.; Brown, G.; Iharchane, S.; et al. Infection and mortality of healthcare workers worldwide from COVID-19: A systematic review. BMJ Glob. Health 2020, 5, e003097. [Google Scholar] [CrossRef]
- Sanghera, J.; Pattani, N.; Hashmi, Y.; Varley, K.F.; Cheruvu, M.S.; Bradley, A.; Burke, J.R. The impact of SARS-CoV-2 on the mental health of healthcare workers in a hospital setting–A Systematic Review. J. Occup. Health 2020, 62, e12175. [Google Scholar] [CrossRef] [PubMed]
- Luo, M.; Guo, L.; Yu, M.; Jiang, W.; Wang, H. The psychological and mental impact of coronavirus disease 2019 (COVID-19) on medical staff and general public—A systematic review and meta-analysis. Psychiatry Res. 2020, 291, 113190. [Google Scholar] [CrossRef]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ (Clin. Res. Ed.) 2020, 369, m1642. [Google Scholar] [CrossRef] [PubMed]
- Xiaoming, X.; Ming, A.; Su, H.; Wo, W.; Jianmei, C.; Qi, Z.; Hua, H.; Xuemei, L.; Lixia, W.; Jun, C.; et al. The psychological status of 8817 hospital workers during COVID-19 Epidemic: A cross-sectional study in Chongqing. J. Affect. Disord. 2020, 276, 555–561. [Google Scholar] [CrossRef] [PubMed]
- Chan, A.O.; Huak, C.Y. Psychological impact of the 2003 severe acute respiratory syndrome outbreak on health care workers in a medium size regional general hospital in Singapore. Occup. Med. 2004, 54, 190–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, K.S.; Shelat, V.G.; Chia, F.L. Psychological impact of the COVID-19 pandemic on training of postgraduate year 1 doctors in Singapore. Singap. Med. J. 2021, 1, 9. [Google Scholar] [CrossRef]
- Chew, Q.H.; Chia, F.L.; Ng, W.K.; Lee, W.C.I.; Tan, P.L.L.; Wong, C.S.; Puah, S.H.; Shelat, V.G.; Seah, E.D.; Huey, C.W.T.; et al. Perceived stress, stigma, traumatic stress levels and coping responses amongst residents in training across multiple specialties during COVID-19 pandemic—A longitudinal study. Int. J. Environ. Res. Public Health 2020, 17, 6572. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Chen, Y.C.; Hsu, S.Y.; Hsieh, H.Y.; Chien, P.C. Defining polytrauma by abbreviated injury scale ≥ 3 for a least two body regions is insufficient in terms of short-term outcome: A cross-sectional study at a level I trauma center. Biomed. J. 2018, 41, 321–327. [Google Scholar] [CrossRef]
- Hsieh, C.H.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Differences between the sexes in motorcycle-related injuries and fatalities at a Taiwanese level I trauma center. Biomed. J. 2017, 40, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, C.H.; Liu, H.T.; Hsu, S.Y.; Hsieh, H.Y.; Chen, Y.C. Motorcycle-related hospitalizations of the elderly. Biomed. J. 2017, 40, 121–128. [Google Scholar] [CrossRef]
- Bandura, A. The Nature and Structure of Self-Efficacy, Self-Efficacy: The Exercise of Control; W.H. Freeman and Co: New York, NY, USA, 1997; pp. 36–78. [Google Scholar]
- Schwarzer, R. Optimistic self-beliefs: Assessment of general perceived self-efficacy in thirteen cultures. Word Psychol. 1997, 3, 177–190. [Google Scholar]
- Luszczynska, A.; Scholz, U.; Schwarzer, R. The general self-efficacy scale: Multicultural validation studies. J. Psychol. 2005, 139, 439–457. [Google Scholar] [CrossRef] [Green Version]
- Andrews, F.M.; Andrews, F.M. Measures of Personality and Social Psychological Attitudes; Academic Press: San Diego, CA, USA, 1991; Volume 1. [Google Scholar]
- Watson, D.; Clark, L.A.; Tellegen, A. Development and validation of brief measures of positive and negative affect: The PANAS scales. J. Personal. Soc. Psychol. 1988, 54, 1063–1070. [Google Scholar] [CrossRef]
- Cecchetto, F.H.; Pellanda, L.C. Construction and validation of a questionnaire on the knowledge of healthy habits and risk factors for cardiovascular disease in schoolchildren. J. Pediatr. 2014, 90, 415–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campos, C.I.; Pitombo, C.S.; Delhomme, P.; Quintanilha, J.A. Comparative analysis of data reduction techniques for questionnaire validation using self-reported driver behaviors. J. Saf. Res. 2020, 73, 133–142. [Google Scholar] [CrossRef]
- Alnaami, N.; Al Haqwi, A.; Masuadi, E. Clinical learning evaluation questionnaire: A confirmatory factor analysis. Adv. Med. Educ. Pract. 2020, 11, 953–961. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, A.; Farmer, E.A.; Greco, M.J. Multisource feedback as part of the Medical Board of Australia’s Professional Performance Framework: Outcomes from a preliminary study. BMC Med. Educ. 2018, 18, 323. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajabi, F.; Pirdehghan, A.; Sanaie, Z.; Ghadirian, L.; Sayarifard, A.; Esna-Ashari, F. Designing and investigating the validity and reliability of the health literacy questionnaire in Iran: Recognizing the risk factors for cardiovascular diseases, diabetes, and cancer. Int. J. Prev. Med. 2020, 11, 110. [Google Scholar] [CrossRef] [PubMed]
- Butterfield, P.S. The stress of residency. A review of the literature. Arch. Intern. Med. 1988, 148, 1428–1435. [Google Scholar] [CrossRef]
- Firth-Cozens, J. Interventions to improve physicians’ well-being and patient care. Soc. Sci. Med. 2001, 52, 215–222. [Google Scholar] [CrossRef]
- Williams, E.S.; Manwell, L.B.; Konrad, T.R.; Linzer, M. The relationship of organizational culture, stress, satisfaction, and burnout with physician-reported error and suboptimal patient care: Results from the MEMO study. Health Care Manag. Rev. 2007, 32, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A.; Caprara, G.V.; Barbaranelli, C.; Pastorelli, C.; Regalia, C. Sociocognitive self-regulatory mechanisms governing transgressive behavior. J. Personal. Soc. Psychol. 2001, 80, 125–135. [Google Scholar] [CrossRef]
- Bandura, A. Health promotion by social cognitive means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- Watson, D. Stability versus change, dependability versus error: Issues in the assessment of personality over time. J. Res. Personal. 2004, 38, 319–350. [Google Scholar] [CrossRef]
- Watson, D.; Wiese, D.; Vaidya, J.; Tellegen, A. The two general activation systems of affect: Structural findings, evolutionary considerations, and psychobiological evidence. J. Personal. Soc. Psychol. 1999, 76, 820–838. [Google Scholar] [CrossRef]
- Bandera, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice Hall: Englewood Cliffs, NJ, USA, 1986. [Google Scholar]
- Maunder, R.; Hunter, J.; Vincent, L.; Bennett, J.; Peladeau, N.; Leszcz, M.; Sadavoy, J.; Verhaeghe, L.M.; Steinberg, R.; Mazzulli, T. The immediate psychological and occupational impact of the 2003 SARS outbreak in a teaching hospital. CMAJ 2003, 168, 1245–1251. [Google Scholar]
- Batra, K.; Singh, T.P.; Sharma, M.; Batra, R.; Schvaneveldt, N. Investigating the psychological impact of COVID-19 among healthcare workers: A meta-analysis. Int. J. Environ. Res. Public Health 2020, 17, 9096. [Google Scholar] [CrossRef]
- Lazarus, R.S.; Folkman, S. Stress Appraisal and Coping; Springer: New York, NY, USA, 1984. [Google Scholar]
- Tyssen, R.; Vaglum, P.; Gronvold, N.T.; Ekeberg, O. The impact of job stress and working conditions on mental health problems among junior house officers. A nationwide Norwegian prospective cohort study. Med. Educ. 2000, 34, 374–384. [Google Scholar] [CrossRef]
- Weinberger, S.E.; Smith, L.G.; Collier, V.U. Redesigning training for internal medicine. Ann. Intern. Med. 2006, 144, 927–932. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | PGY Training | p | |
|---|---|---|---|
| Yes (n = 77) | No (n = 33) | ||
| Age (years) | <0.001 | ||
| 21–30, n (%) | 52 (67.5) | 3 (9.1) | |
| 31–40, n (%) | 18 (23.4) | 6 (18.2) | |
| 41–50, n (%) | 7 (9.1) | 16 (48.5) | |
| ≥51, n (%) | 0 (0.0) | 8 (24.2) | |
| Seniority | <0.001 | ||
| PGY, n (%) | 46 (59.7) | 0 (0.0) | |
| Resident, n (%) | 13 (16.9) | 5 (15.2) | |
| Junior vs., n (%) | 15 (19.5) | 6 (18.2) | |
| Senior vs., n (%) | 3 (3.9) | 22 (66.6) | |
| Practice experience | <0.001 | ||
| <1 year, n (%) | 44 (57.1) | 1 (3.0) | |
| 1–9 years, n (%) | 24 (31.2) | 7 (21.2) | |
| 10–19 years, n (%) | 9 (11.7) | 15 (45.5) | |
| ≥20 years, n (%) | 0 (0.0) | 10 (30.3) | |
| Experience caring for patients with SARS | <0.001 | ||
| No, n (%) | 60 (77.9) | 9 (27.3) | |
| Yes, n (%) | 17 (22.1) | 24 (72.7) | |
| Experience caring for patients with COVID-19 | 0.027 | ||
| No, n (%) | 49 (63.6) | 11 (33.3) | |
| Yes, n (%) | 28 (36.4) | 22 (66.7) | |
| Variables | PGY (n = 46) | Resident (n = 18) | Junior vs. (n = 21) | Senior vs. (n = 25) | p |
|---|---|---|---|---|---|
| Ability to cope with ease | −0.45 ± 0.97 | 0.07 ± 0.83 | 0.38 ± 0.60 | 0.47 ± 0.71 | <0.001 |
| Proactive ability | −0.18 ± 0.87 | −0.10 ± 1.02 | 0.04 ± 0.75 | 0.37 ± 0.92 | 0.09 |
| Negative emotion | 0.16 ± 0.93 | −0.02 ± 1.07 | −0.09 ± 0.77 | −0.20 ± 1.10 | 0.49 |
| Positive emotion | −0.19 ± 0.99 | −0.29 ± 0.89 | 0.23 ± 0.80 | 0.37 ± 0.92 | 0.04 |
| Variables | PGY Training | p | |
|---|---|---|---|
| Yes (n = 77) | No (n = 33) | ||
| Ability to cope with ease | 0.50 ± 0.69 | −0.22 ± 0.92 | 0.001 |
| Proactive ability | 0.21 ± 0.86 | −0.09 ± 0.81 | 0.009 |
| Negative emotion | −0.07 ± 0.97 | 0.03 ± 0.97 | 0.630 |
| Positive emotion | 0.33 ± 0.92 | −0.14 ± 0.94 | 0.020 |
| Variables | Experience Caring for Patients with SARS | p | |
|---|---|---|---|
| Yes (n = 41) | No (n = 69) | ||
| Ability to cope with ease | 0.33 ± 0.78 | −0.19 ± 0.94 | 0.004 |
| Proactive ability | 0.29 ± 0.79 | −0.17 ± 0.92 | 0.006 |
| Negative emotion | −0.17 ± 1.00 | 0.10 ± 0.94 | 0.151 |
| Positive emotion | 0.29 ± 0.90 | −0.17 ± 0.95 | 0.014 |
| Variables | Experience Caring for patients with SARS | p | |
|---|---|---|---|
| Yes (n = 26) | No (n = 24) | ||
| Ability to cope with ease | 0.29 ± 0.76 | −0.16 ± 0.78 | 0.045 |
| Proactive ability | 0.46 ± 0.74 | 0.03 ± 0.58 | 0.026 |
| Negative emotion | −0.23 ± 0.76 | 0.03 ± 0.78 | 0.232 |
| Positive emotion | 0.43 ± 0.87 | −0.19 ± 0.72 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-H.; Cheng, Y.-H.; Shen, Y.-C.; Kung, C.-T.; Chien, P.-C.; Hsieh, C.-H. The Effect of Post-Graduate Year Training on the Self-Efficacy and Emotional Traits of Physicians Facing the COVID-19 Pandemic. Healthcare 2021, 9, 912. https://doi.org/10.3390/healthcare9070912
Chen C-H, Cheng Y-H, Shen Y-C, Kung C-T, Chien P-C, Hsieh C-H. The Effect of Post-Graduate Year Training on the Self-Efficacy and Emotional Traits of Physicians Facing the COVID-19 Pandemic. Healthcare. 2021; 9(7):912. https://doi.org/10.3390/healthcare9070912
Chicago/Turabian StyleChen, Chih-Hung, Ya-Hui Cheng, Yuan-Chi Shen, Chia-Te Kung, Peng-Chen Chien, and Ching-Hua Hsieh. 2021. "The Effect of Post-Graduate Year Training on the Self-Efficacy and Emotional Traits of Physicians Facing the COVID-19 Pandemic" Healthcare 9, no. 7: 912. https://doi.org/10.3390/healthcare9070912