1. Introduction
Globally, cranioencephalic trauma affects an estimated 200 individuals out of 10,000, with a higher prevalence among men in a ratio of 3:2, particularly within the age range of 20 to 30, possibly due to increased engagement in sports and high-risk activities [
1]. Industrialized nations report falls from one’s own height as the leading cause (60% of cases), alongside traffic accidents and acts of violence, collectively contributing to a 3.4% mortality rate [
2,
3]. In Latin America, head trauma is predominantly linked to traffic accidents (motorcyclists and pedestrians) and violence (internal guerrilla conflicts) [
4]. In Colombia, limited demographic studies focus on the incidence of mild or moderate traumatic brain injury, situations often requiring cranial implants. Research in Cali between 2003 and 2004 indicated that 52% and 30% of admitted traumatic brain injury cases were categorized as mild and moderate, respectively [
5]. The mortality rate in Colombia for the period 2010–2017 was 10.7 per 100,000 inhabitants [
6].
Biomechanics is a multidisciplinary field that plays a crucial role in addressing bone injuries and defects, particularly in the development of orthopedic implants. These implants, made from a variety of biomaterials, are essential for proper bone alignment and healing [
7]. To enhance the interaction between these implants and bone tissue, bioinspired surface modifications are being explored, with the aim of creating next-generation implants [
8]. The biomechanics of bone fractures and fixation, including the use of implants, is a key area of study in orthopedic trauma [
9]. Orthopedic implant studies encompass design, new materials, and physiology [
10,
11]. To ensure the final product effectively restores the functionality of the missing biological structure, these disciplines must collaborate [
12]. Engineering is vital in evaluating prototype designs, identifying flaws, refining implants, and assuring patients of improved quality of life.
For over 80 years, scientists have been investigating and evaluating various synthetic biomaterials to address cranial defects [
12], and the exploration for new materials, including those with biodegradable features, continues [
13]. Among them, we find PMMA, a polymethylmethacrylate ceramic mixed with a liquid monomer, which passes from a liquid system to a non-Newtonian one to end up solidifying, through an exothermic energetic release process, in the form desired by the orthopedist. PMMA is a durable, malleable, and relatively inexpensive biomaterial [
14], very efficient in aesthetic terms for sealing asymmetric and extensive defects, with great properties for surgical use [
15]. PMMA has demonstrated remarkable success rates exceeding 97% and boasts a notably low complication rate of less than 2.3% [
16,
17]. Inconveniences have also been reported due to the low porosity of PMMA implants, since it does not favor the cell growth of osteocytes, nor does it facilitate its vascularization, creating an inert material susceptible to infection, although the literature reports less than 5% of infections with this biomaterial [
18]. Finally, low mechanical properties are attributed to it in terms of tensile strength (36 MPa), 4.7 times less than cortical bone (170 MPa) [
19], which raises doubts in surgeons when assessing its mechanical strength and stiffness, especially considering that many of these patients may be at risk of experiencing significant impacts.
Currently, surgeons have put their interest in PEEK (Polyether Ether Ketone), a thermally stable biomaterial [
20] with success rates exceeding 99% [
21], as indicated by studies. This biomaterial boasts low post-surgical complication rates ranging from 0% to 9% [
16,
22], and infection-related complications are less than 6% [
23,
24]. Moreover, PEEK exhibits a tensile strength of 80 MPa, two times lower than cortical bone strength. These attributes position PEEK as a promising biomaterial for surgical applications, presenting a high success rate, low complication rates, and advantageous mechanical properties when compared to alternative materials like PMMA.
Both biomaterials exhibit comparable clinical success rates, low complication rates, low infection rates, and high aesthetic satisfaction reported by patients [
22], making them seemingly suitable for shielding the brain from mechanical trauma. However, they diverge in mechanical properties and costs, with PMMA being approximately 55% more economical than PEEK (USD 2702 vs. USD 4684, approximate value for an implant in Colombia without osteosynthesis material). In [
25], the authors proposed an integrative surgery management system for cranial reconstructions using patient-specific implants made of PMMA as an accessible and cost-effective solution for low-income countries. This cost differential underscores a significant economic consideration in choosing between the two materials for neurosurgical implants while maintaining comparable clinical effectiveness and patient satisfaction.
The digitization of medical implants and their subsequent analysis using computational mechanics, such as finite element (FE) analysis, has significantly advanced the exploration and investigation of implant design [
26,
27]. These tools allow engineers to evaluate various parameters, including thickness, geometrical features, thermal properties, materials, and applied boundary conditions. This enables the creation of more customized implants from a mechanical perspective, blending the most favorable attributes to ensure prolonged implant durability [
28]. Computational modeling and simulation play a crucial role in the total product life cycle of implants, analyzing both surgical procedures and devices, taking into account the topics of both hard and soft tissue mechanics.
Research using FE analysis has been reported applied to cranial implants evaluating the variable thickness vs. type of material, where it has been concluded that the thickness factor is more relevant to stresses than the material used for its manufacture. However, the situation differs when it comes to deformation, and the elastic modulus of the material significantly affects the displacement field. In another set of experiments, researchers evaluated the stress–strain behavior of two types of cranial implants, titanium (Ti) and PEEK, under axial loading [
29]. Special interest has been given to the geometric shape of the system of miniplates that hold the implant–skull interface and how these react to different types of loads [
30,
31]. In general, there has been a surge in research within the literature employing FE approaches to evaluate cranial implants [
32,
33,
34,
35], driven by a heightened interest in the subject. In [
32], the authors employed finite element analysis to assess implant behavior under varied intracranial pressure conditions, considering the influence of fixation points, for different materials. The study in [
33] models cranial implants with meshless methods, comparing solid and porous structures, for titanium alloy (Ti6Al4V) and PEEK, indicating titanium’s overall superiority, while PEEK excels in weight and osseointegration. In [
35], evaluation of von Mises stresses and deformations in a customized PMMA-based cranial implant with the fixation system demonstrated effective protection without physiological harm or anchoring failures.
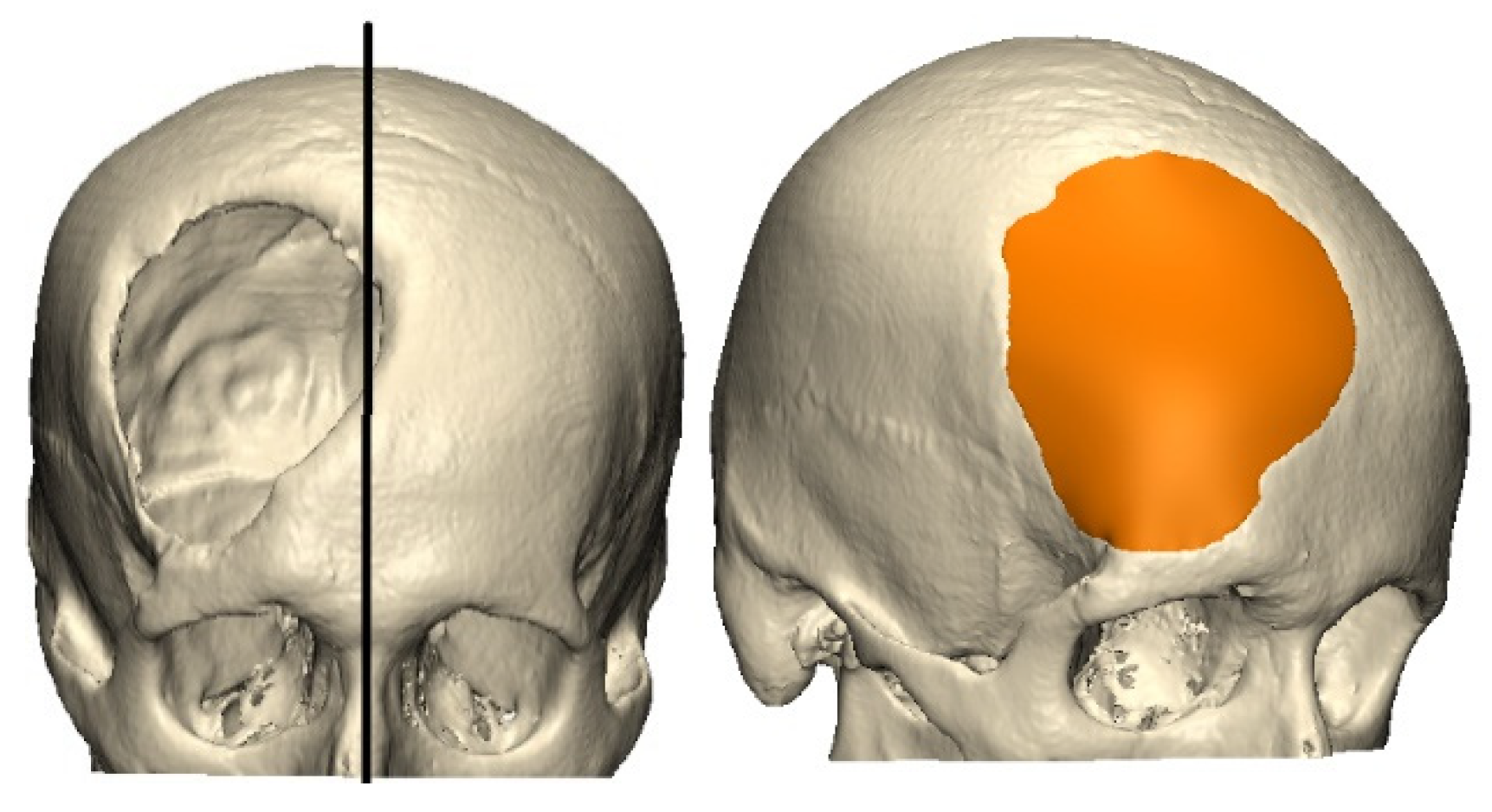
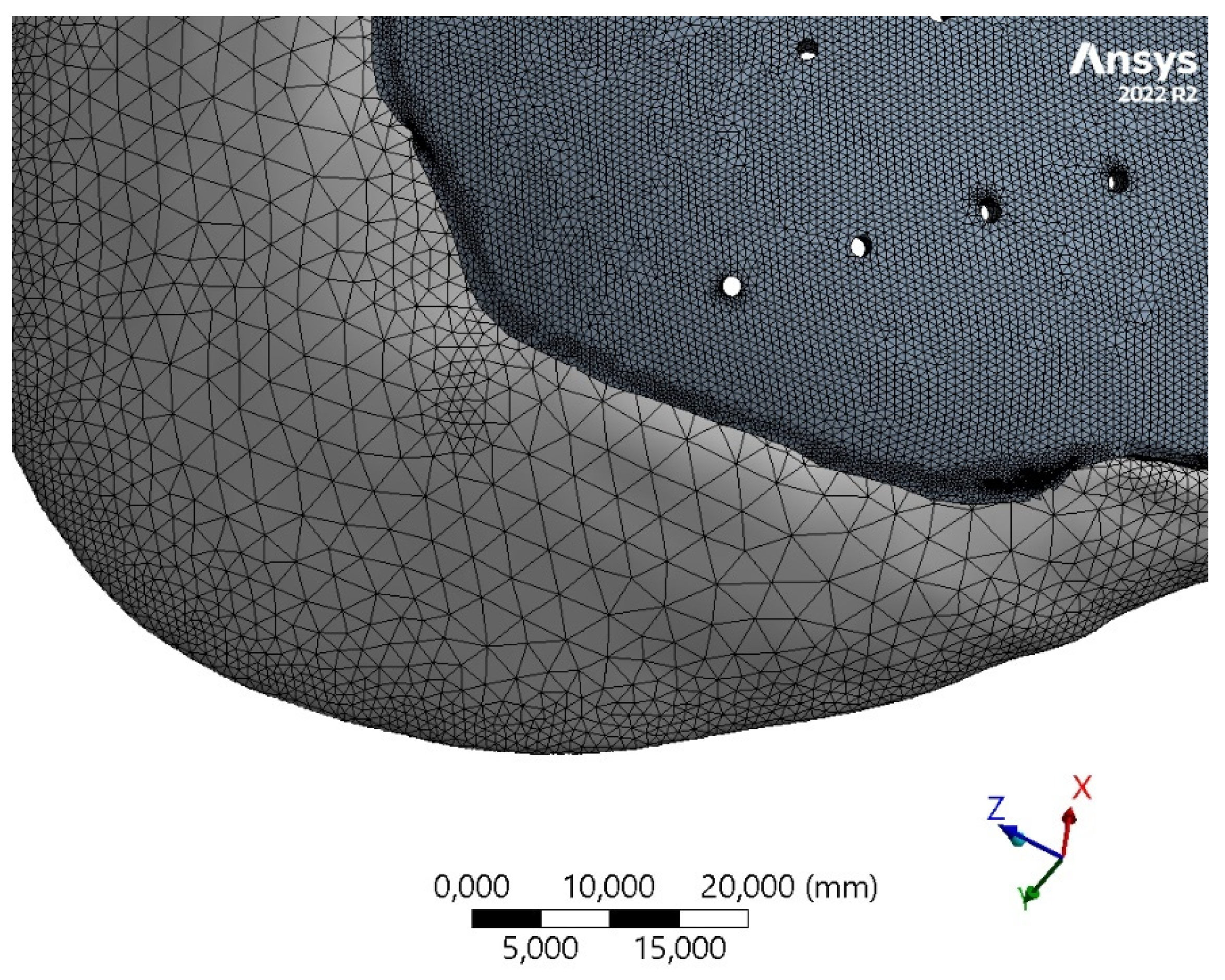
This work presents the study of the thickness vs. stiffness relationship for different materials (PMMA and PEEK), as a criterion for the selection of biomaterials from a mechanical perspective. Our null hypothesis is that the two biomaterials offer the minimum mechanical characteristics to withstand a direct impact trauma in the geometric center of the implant, e.g., as a result of a ball impact, and avoid critical deformations greater than 2 mm. In this way, the use of PMMA cranioplasties is justified in most cases where a PEEK implant cannot be accessed. First, the subject for the study is presented. Leveraging a computed tomography (CT) scan, we extract essential spatial and topological data, forming the foundation for precise model identification. Next, we continue with the design of a patient-specific implant, tailoring the solution to the individual’s unique anatomical characteristics. Finally, the structural integrity of the implant is assessed through finite element analysis, providing comprehensive insights into its performance under varying conditions, including material, topology, and thickness.
3. Results
In our study, a
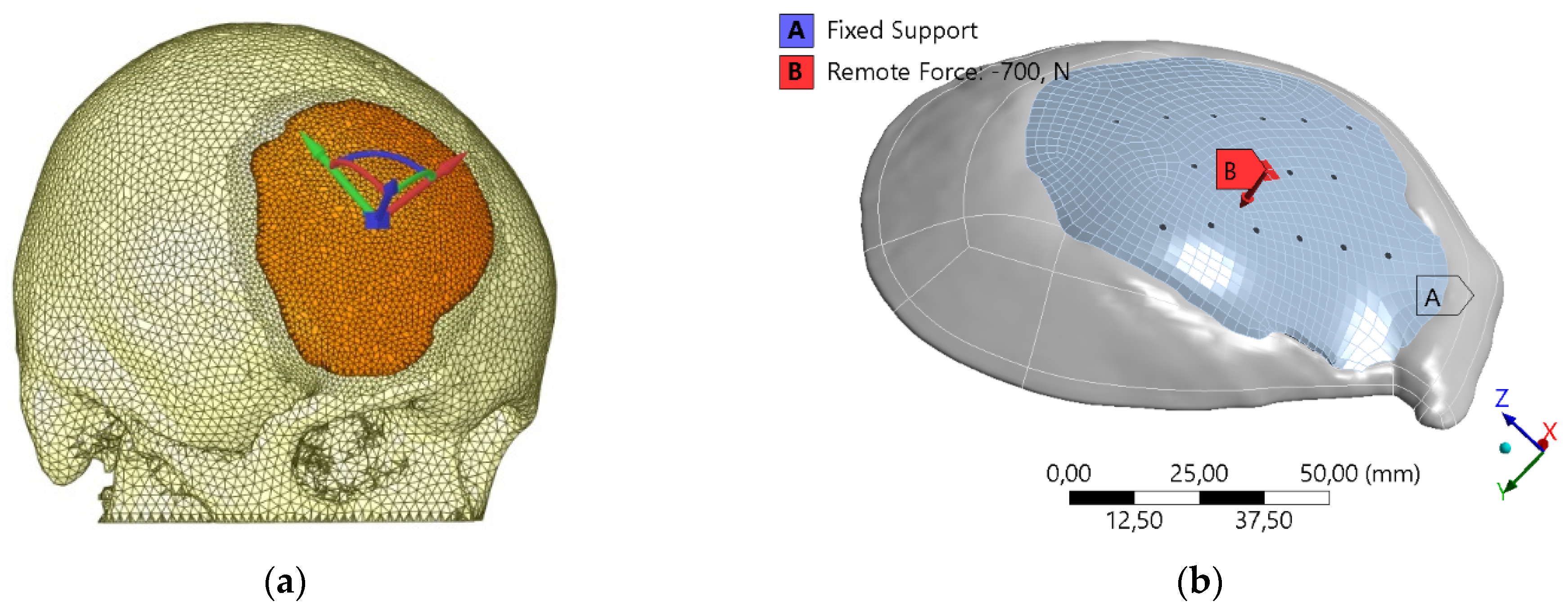
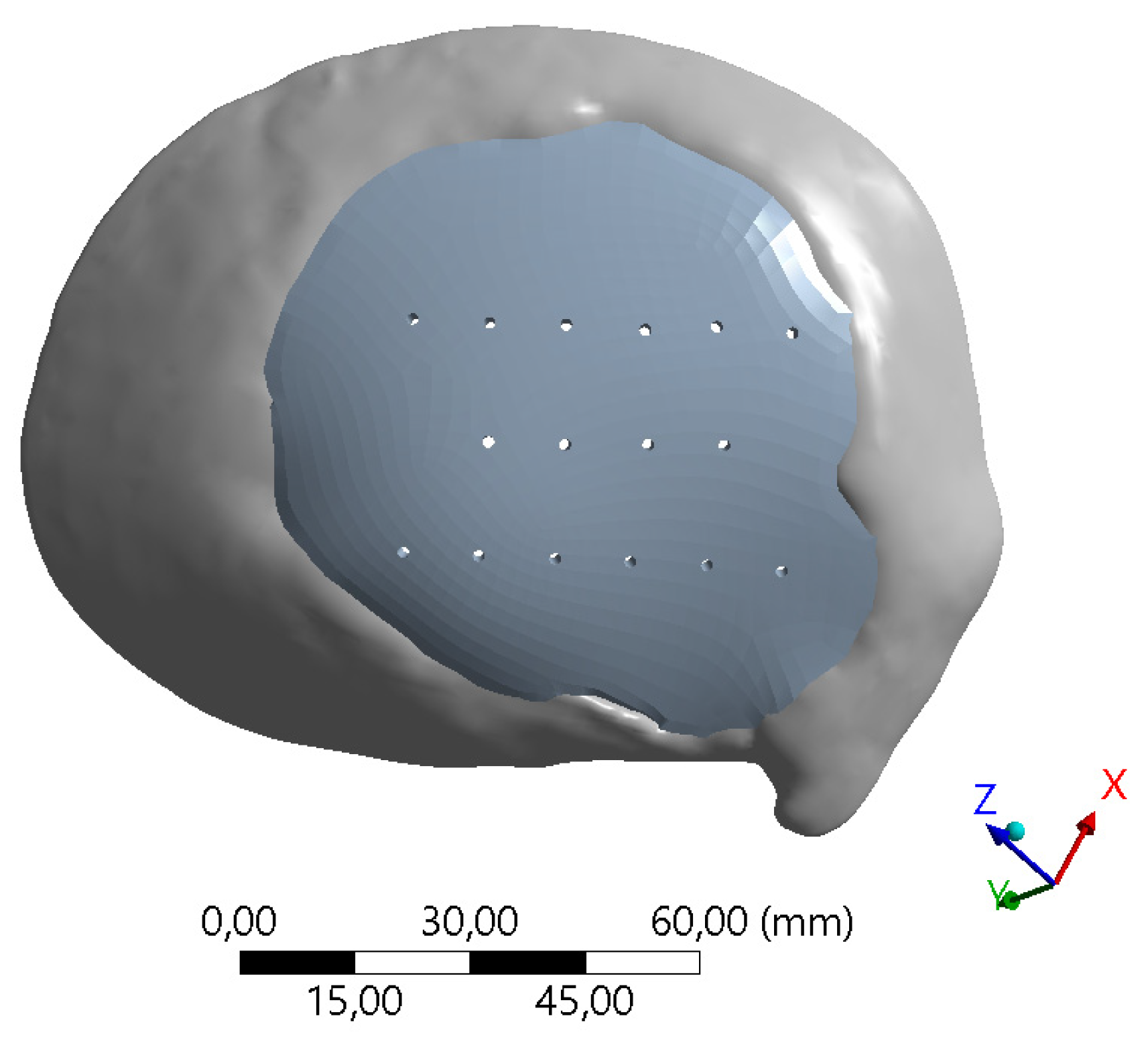
factorial experiment was undertaken to examine the impacts of material type (PEEK and PMMA), implant thickness (3 mm and 5 mm), and the presence of perforations for suturing (with and without) on cranial implant performance. This design resulted in eight experimental runs, encompassing all possible combinations of these factors. The response variable, indicating the primary outcome (i.e., maximum displacement), was measured for each experimental run. Employing statistical analysis, we assessed the main effects and potential interactions among these factors, aiming to discern the influence of material choice, thickness variations, and the presence of perforations on the properties of cranial implants. The findings contribute valuable insights into optimizing cranial implant design based on these critical factors. The results of the eight experiments are presented in
Table 5, which shows the maximum total displacements for different implant configurations.
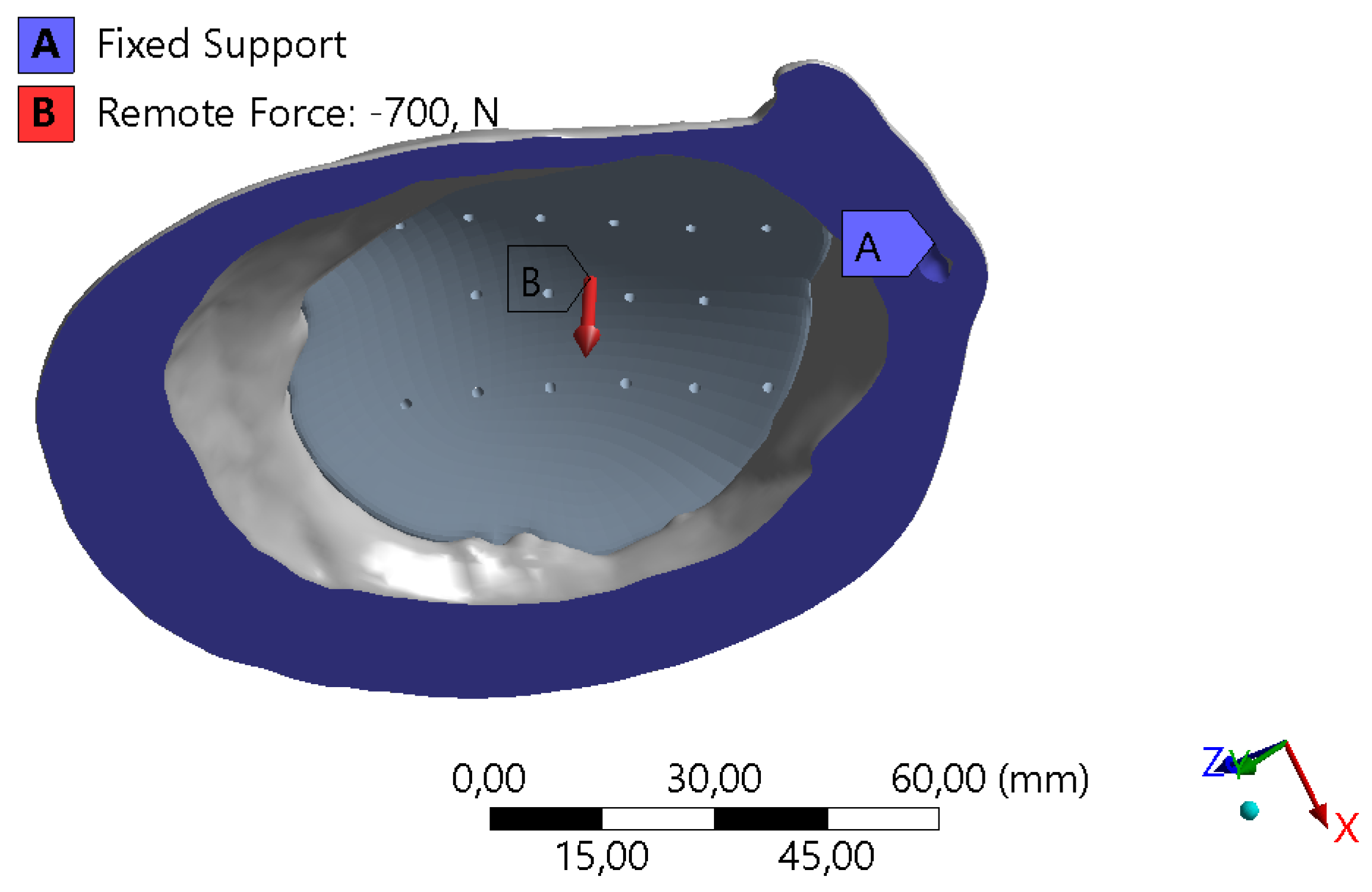
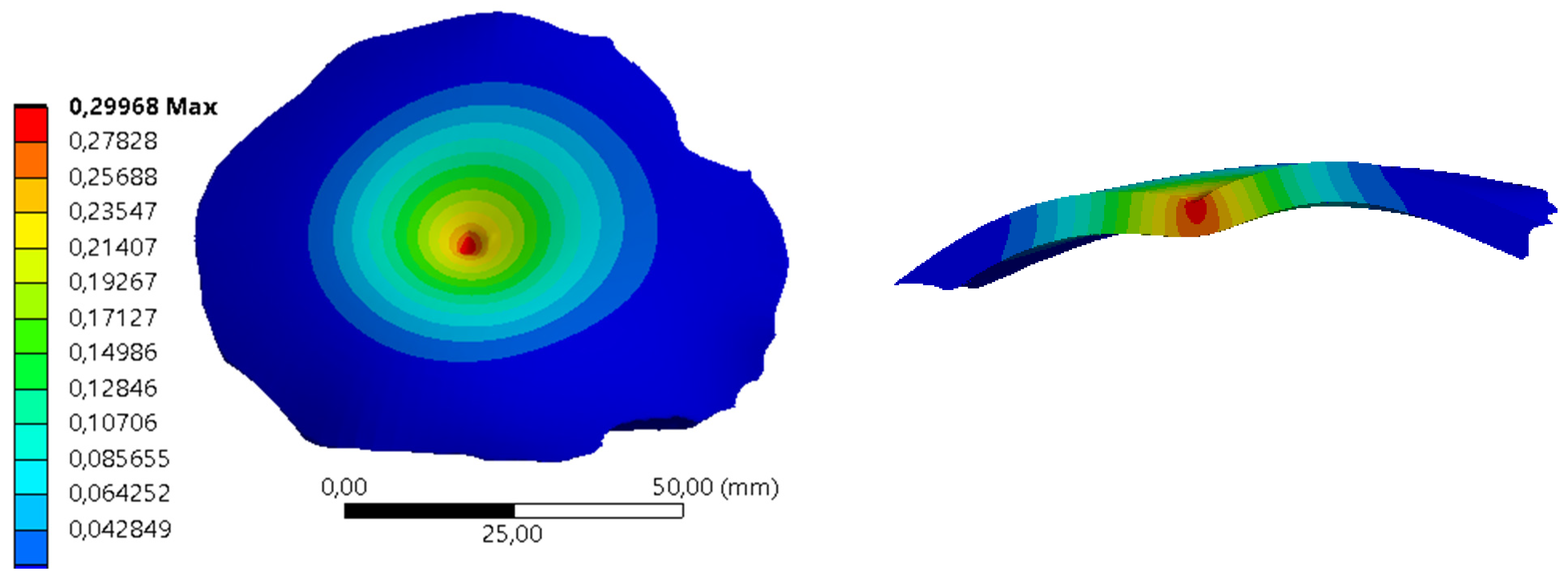
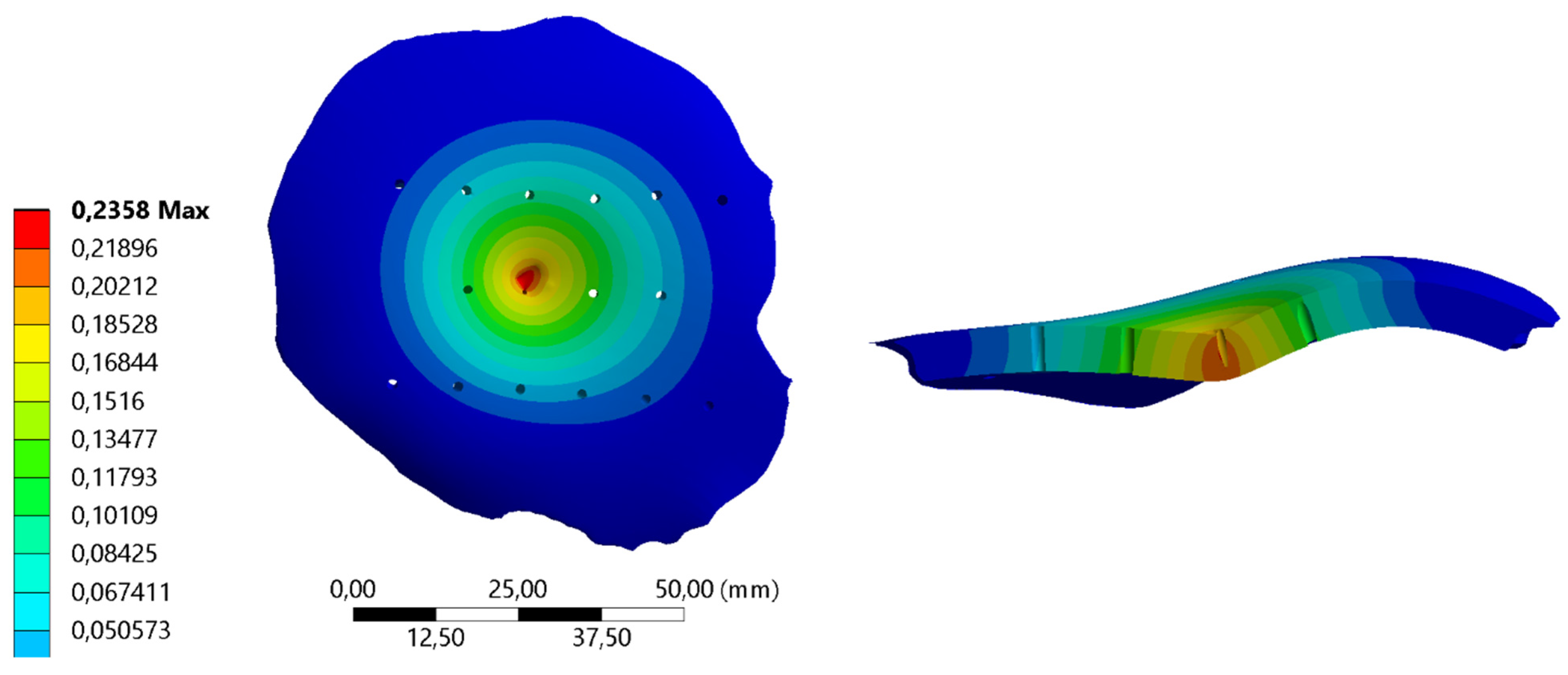
Figure 6 and
Figure 7 show the total displacements for the implants under a load of 700 N applied on the apex of the implant for two experiments of the different configurations of biomaterial, thickness, and perforations.
The effect that each one of the factors studied has on the normal displacements of the surface is presented in
Table 6. The results of our study revealed several key findings regarding the main effects and interactions of factors on our experimental outcome. Regarding the main effects, implant thickness exhibited a notable negative effect with a coefficient of −0.684 (±0.01), indicating that increasing implant thickness was associated with a decrease in the observed outcome. Conversely, the choice of biomaterial showed a positive effect of 0.193 (±0.01), suggesting that certain biomaterials, i.e., PMMA, were associated with higher outcomes. Perforations, as a main effect, had a minimal effect with a coefficient of 0.022 (±0.01). In terms of two-factor interactions, the interaction between thickness and biomaterial showed a negative effect of −0.116 (±0.01), suggesting that the combination of certain thicknesses and biomaterials led to a reduction in the outcome. The interactions between thickness and perforations (−0.008 ± 0.01) and biomaterial and perforations (0.004 ± 0.01) had relatively minor effects on the observed outcome. These results provide insights into the complex interplay between implant characteristics and their impact on our experimental outcome.
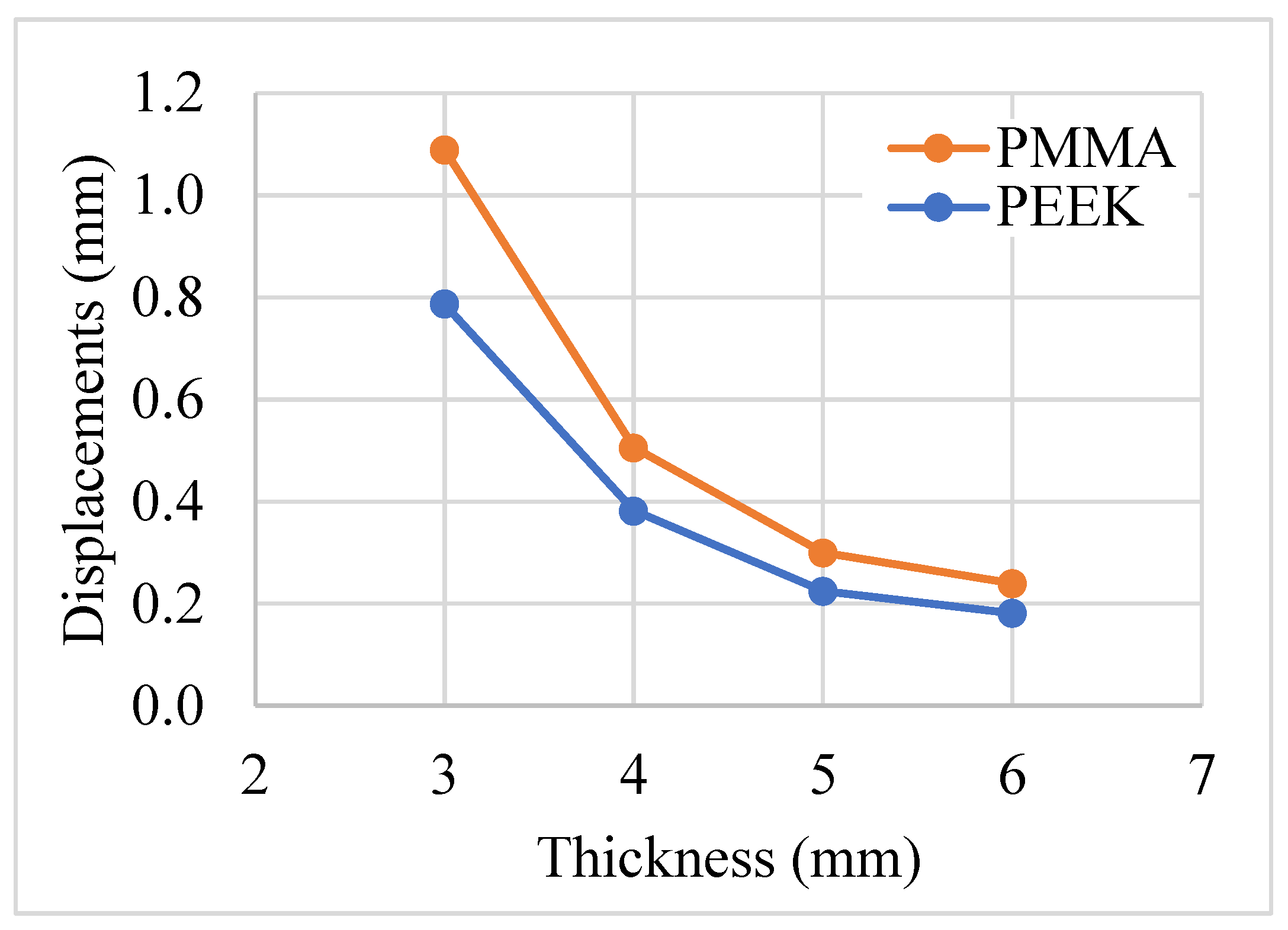
The perforations or holes variable does not seem to have a noticeable influence on the deformations of the implant when the biomaterial is PMMA. Otherwise, when the biomaterial is PEEK, and the thickness is 3 mm, this combination seems to influence the displacements. In the configuration of change of thickness and biomaterial, it is observed that for thicknesses of 3 mm the biomaterial influences, but for thicknesses of 5 mm, it is not significant. The largest deformation was observed in the combination of 3 mm thickness, PMMA biomaterial, and holes with a displacement of 1.125 mm. In consideration of the influence of thickness, we have included data corresponding to thickness values of 4 mm and 6 mm. This addition is intended to facilitate a comprehensive understanding of the relationship between displacement and thickness increment. The influence of the thickness on the normal displacements to the surface in different combinations of biomaterials is presented in
Figure 8. Comparing the displacement values between PMMA and PEEK implants at each thickness level, it appears that PEEK generally exhibits lower displacement values than PMMA, and the difference diminishes as we increase the thickness. The displacement decreases non-linearly with thickness for both materials, and when considering displacement as proportional to the elastic modulus, these findings align with the ratio of their respective elastic moduli. These findings can inform clinical decisions regarding the selection of implant materials and thicknesses based on desired mechanical performance and patient-specific factors such as bone quality and surgical requirements.
4. Conclusions
In this study, we investigated the relationship between implant thickness and deformation, focusing on patient-specific cranial implants constructed from two different biomaterials, PMMA and PEEK. Our goal was to assess their mechanical performance under quasi-static loads, particularly in terms of maximum total deformation. While the paper explores readily accessible techniques, its main objective is to address the cost-benefit aspects of employing PMMA implants in clinical applications, particularly in comparison to more expensive alternatives, an aspect that has not been previously explored in the literature. Our experience indicates that this matter lacks clarity for practitioners, and its relevance is notably significant in developing countries. Achieving a comprehensive grasp of the materials and their mechanical performance is relevant in this context. The outcomes of this research shed light on several crucial aspects of implant design and selection. As expected, the choice of biomaterial significantly impacts the deformation characteristics of cranial implants. We observed that PMMA and PEEK exhibit different levels of normal displacements due to their different elastic moduli. Generally, biomaterials with higher elastic moduli experience less deformation under equivalent stress conditions.
Our study adds a practical dimension to existing research [
49] by considering implant perforations as an important factor in surgical procedures. Moreover, we did not consider implants thinner than 3 mm because the fabrication of these implants, generally by the biomaterial injection technique, are difficult to perform for clinical use. In comparison to previous literature, our findings diverge in terms of deformation outcomes. Díaz et al. [
38] report displacements of 0.3 mm in PEEK biomaterial for a cranioplasty in the upper part of the cranial vault, although the implant thickness is not reported. Ridwan-Pramana et al. [
50] report displacements less than 0.03 mm in specific configurations of several plates and positive contact angles between implant and skull; we understand that the other configurations are idealized and do not represent, in many cases, the real topological conditions of these defects in surgery. Finally, it is known that the perpendicular distance between the cranial tissue and the bone plate is around 2 mm [
48,
51]. For this reason, a deformation of the material close to this length would be critical. This deformation is closely linked to the thickness and material of the implant [
49]. Thus, it is necessary for future research to include geometric variables, such as the radius of curvature of the implant. This will allow for a more precise standardization of results, catering to specific implant geometries and providing a more comprehensive understanding of implant performance. The finite element models employed in this study recreated real-life implant conditions under direct impacts, although the osteosynthesis system was not included.
This research validates the null hypothesis that both PMMA and PEEK biomaterials are suitable for withstanding deformation in the normal direction. Furthermore, we found that by adjusting the thickness variable in PMMA biomaterial, deformation levels comparable to those of PEEK can be achieved. These results suggest the potential for PMMA implants, particularly 4 mm thick with perforations, to serve as an effective alternative to PEEK implants, offering a cost-effective solution while maintaining the desired mechanical performance in cranial implants. However, further research and validation are essential to confirm the feasibility and clinical implications of these findings.
While the study enhances understanding of cranial implant performance, limitations exist. Focusing on quasi-static loads excludes dynamic conditions, and implants thinner than 3 mm were omitted. Idealized assumptions about perforations may oversimplify surgical scenarios. Future research should explore geometric variables, incorporate dynamic conditions, explore thinner implants, and integrate osteosynthesis systems for a more realistic analysis. Clinical validation is crucial to confirm practical implications. Despite these limitations, the study suggests the potential of cost-effective PMMA implants as comparable alternatives to PEEK implants, emphasizing the need for further research and validation in clinical settings.


 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}