
A Case Report of Secondary Glaucoma in a Patient with HTLV-1: Discussion about the Management of Secondary Glaucoma Due to Recurrent Granulomatous Uveitis
 and
and
Abstract
:1. Introduction
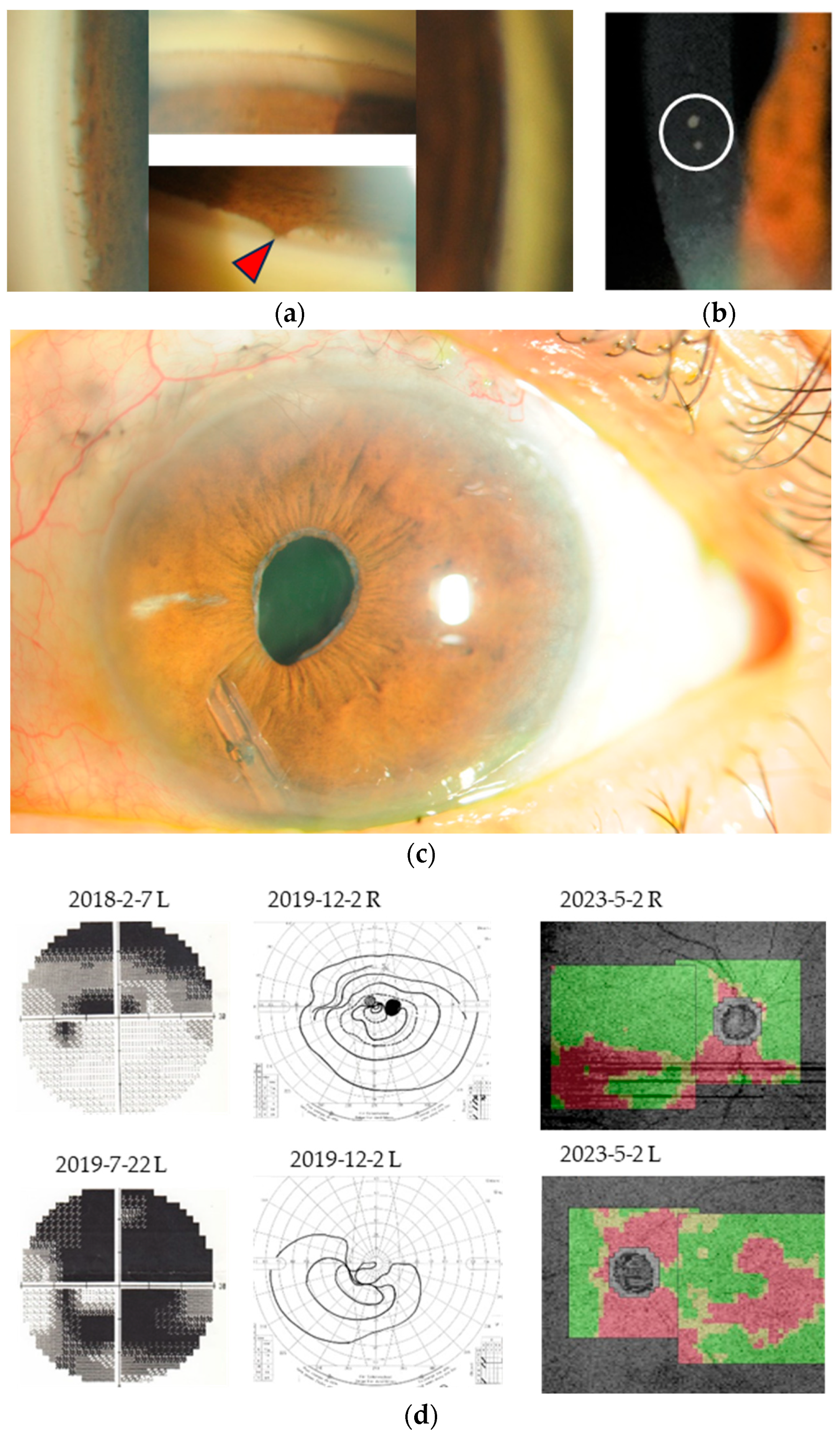
2. Case Report
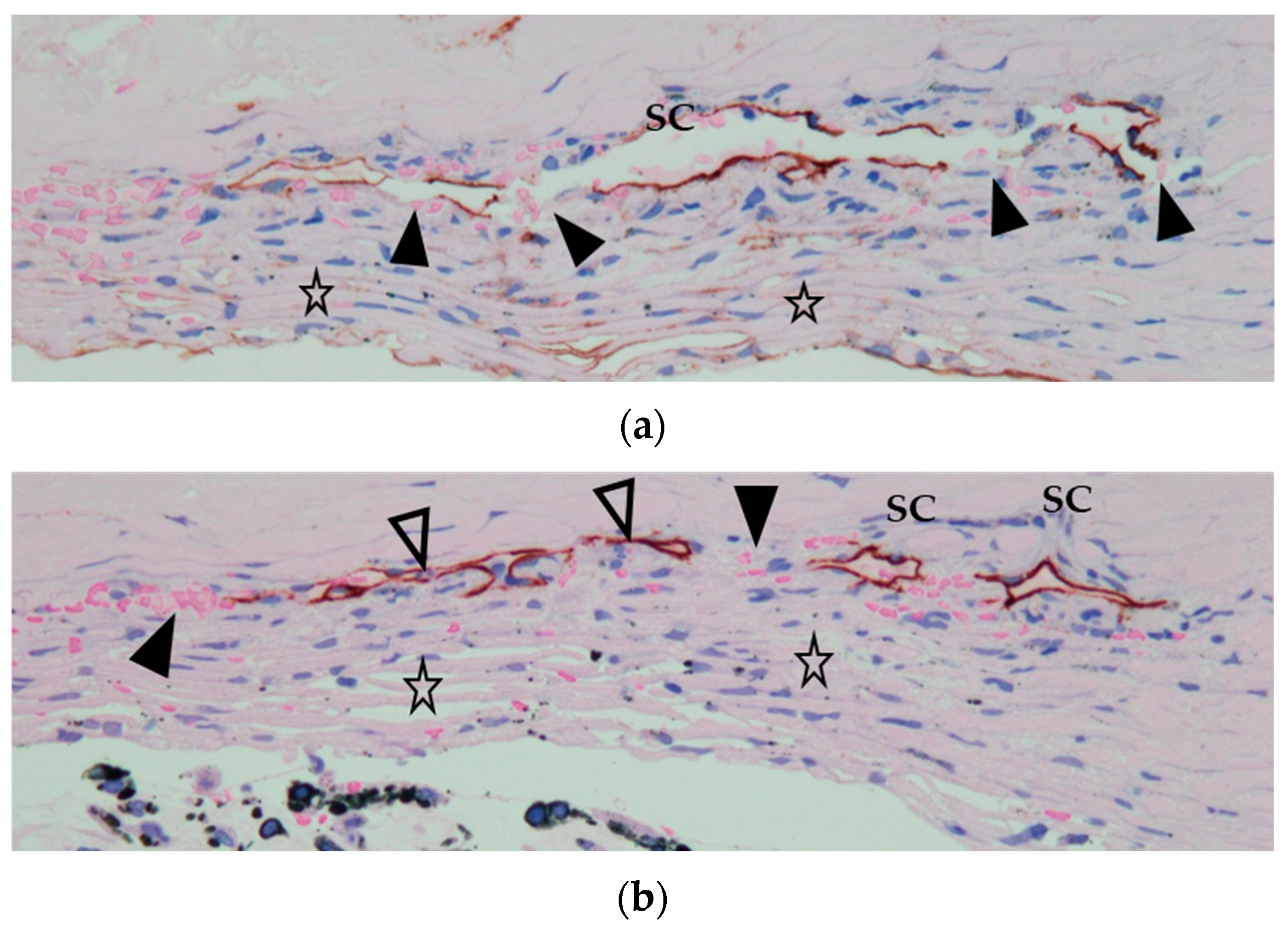
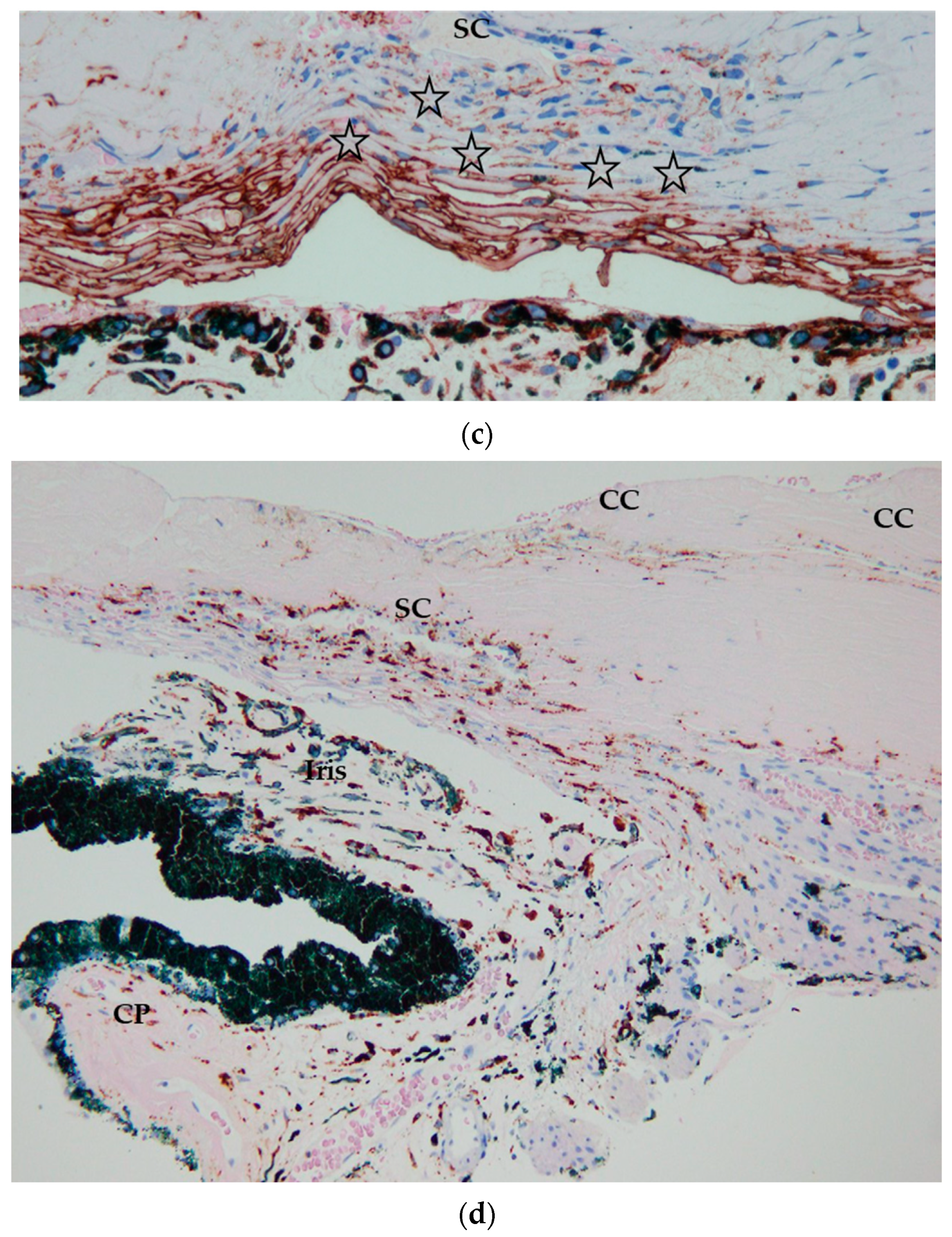
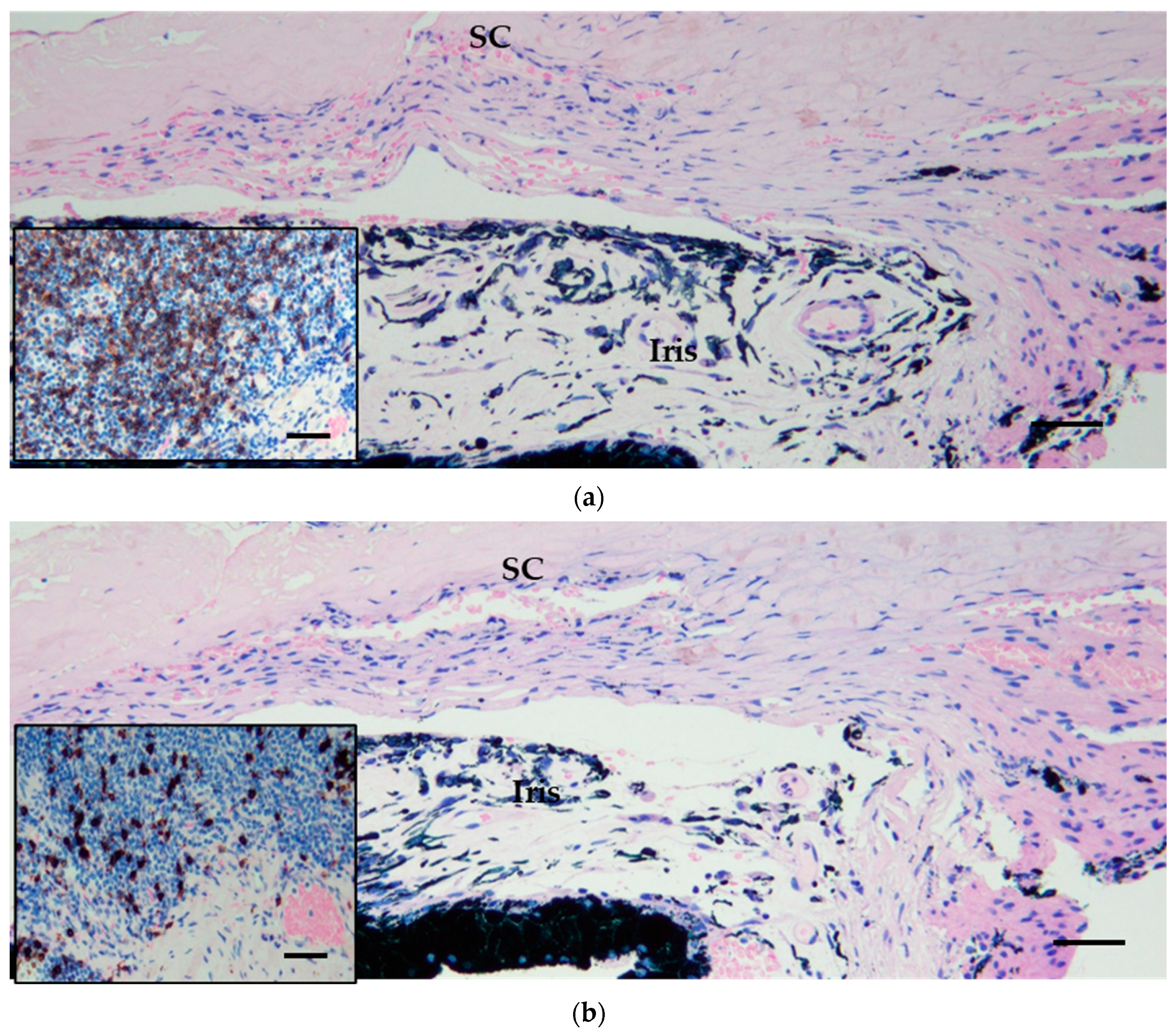
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ohba, N.; Matsumoto, M.; Sameshima, M.; Kabayama, Y.; Nakao, K.; Unoki, K.; Uehara, F.; Kawano, K.; Maruyama, I.; Osame, M. Ocular manifestations in patients infected with human T-lymphotropic virus type I. Jpn. J. Ophthalmol. 1989, 33, 1–12. [Google Scholar] [PubMed]
- Nakao, K.; Matsumoto, M.; Ohba, N. Seroprevalence of antibodies to HTLV-I in patients with ocular disorders. Br. J. Ophthalmol. 1991, 75, 76–78. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, M.; Watanabe, T.; Yamaguchi, K.; Takatsuki, K.; Yoshimura, K.; Shirao, M.; Nakashima, S.; Mori, S.; Araki, S.; Miyata, N. HTLV-I uveitis: A distinct clinical entity caused by HTLV-I. Jpn. J. Cancer Res. 1992, 83, 236–239. [Google Scholar] [CrossRef] [PubMed]
- Mochizuki, M.; Yamaguchi, K.; Takatsuki, K.; Watanabe, T.; Mori, S.; Tajima, K. HTLV-I and uveitis. Lancet 1992, 339, 1110. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, E.; Ono, A.; Hikita, N.; Arima, K.; Mochizuki, M.; Yamaguchi, K.; Tajima, K.; Kiyokawa, H. Estimated Prevalence Rate of HTLV-I Uveitis in Chikugo. J. Jpn. Ophthalmol. Soc. 1998, 102, 327–332. [Google Scholar]
- Terada, Y.; Kamoi, K.; Komizo, T.; Miyata, K.; Mochizuki, M. Human T Cell Leukemia Virus Type 1 and Eye Diseases. J. Ocul. Pharmacol. Ther. 2017, 33, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Kamoi, K.; Mochizuki, M. Human T-Cell Leukemia Virus Type 1. In Emerging Infectious Uveitis; Chee, S.-P., Khairallah, M., Eds.; Springer International Publishing: Cham, Switzerland, 2017; pp. 143–148. [Google Scholar]
- Nakao, K.; Ohba, N. Clinical features of HTLV-I associated uveitis. Br. J. Ophthalmol. 1993, 77, 274–279. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, S.; Hamanaka, T.; Sakurai, T.; Kobayashi, K.; Ishida, N.; Ebihara, N. Evaluation of the outcome of long-tube shunt implant surgery in uveitic glaucoma patients by analyzing the background of uveitis. Int. Ophthalmol. 2021, 41, 509–517. [Google Scholar] [CrossRef] [PubMed]
- Shahnaz, S.; Reich, D.; Arévalo-Valencia, D.; Kucinska, S.; Tulczynska, J.; Fleischman, J. HTLV-1-Associated Adult T Cell Leukemia Lymphoma Presenting as Granulomatous Pneumocystis Jiroveci Pneumonia (PJP) and Hypercalcemia. J. Gen. Intern. Med. 2007, 22, 420–423, PMCID:PMC1824742. [Google Scholar] [CrossRef] [PubMed]
- Hamanaka, T.; Akabane, N.; Sakurai, T.; Ikushima, S.; Kumasaka, T.; Takemura, T. Microangiopathy in Ocular Sarcoidosis Using Fluorescein Gonio and Fundus Angiography from Diagnostic and Therapeutic Aspects. Diagnostics 2021, 11, 39. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| VA (R) | VA (L) | IOP (R) | IOP (L) | |
|---|---|---|---|---|
| 7 January 2019 | 1.0 | 30 cm CF | 23 | 56 |
| 18 March 2019 | 1.2 | 0.01 | 17 | 12 |
| 29 July 2019 | 0.9 | 0.01 | 14 | 9 |
| 2 December 2019 | 0.9 | 0.01 | 14 | 12 |
| 2 March 2020 | 0.9 | 20 cm CF | 21 | 14 |
| 24 April 2023 | / | / | 32 | 12 |
| 8 May 2023 | 0.5 | 20 cm CF | 10 | 8 |
| 26 June 2023 | 0.6 | HM | 16 | 14 |
| 14 July 2023 | 0.8 | HM | 10 | 8 |
| 22 January 2024 | 0.6 | HM | 15 | 13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ashikaga, K.; Hamanaka, T.; Hosogai, M.; Tanaka, T.; Nakao, S.; Funaki, T. A Case Report of Secondary Glaucoma in a Patient with HTLV-1: Discussion about the Management of Secondary Glaucoma Due to Recurrent Granulomatous Uveitis. J. Clin. Transl. Ophthalmol. 2024, 2, 26-33. https://doi.org/10.3390/jcto2020003
Ashikaga K, Hamanaka T, Hosogai M, Tanaka T, Nakao S, Funaki T. A Case Report of Secondary Glaucoma in a Patient with HTLV-1: Discussion about the Management of Secondary Glaucoma Due to Recurrent Granulomatous Uveitis. Journal of Clinical & Translational Ophthalmology. 2024; 2(2):26-33. https://doi.org/10.3390/jcto2020003
Chicago/Turabian StyleAshikaga, Kenta, Teruhiko Hamanaka, Mayumi Hosogai, Takao Tanaka, Shintaro Nakao, and Toshinari Funaki. 2024. "A Case Report of Secondary Glaucoma in a Patient with HTLV-1: Discussion about the Management of Secondary Glaucoma Due to Recurrent Granulomatous Uveitis" Journal of Clinical & Translational Ophthalmology 2, no. 2: 26-33. https://doi.org/10.3390/jcto2020003