
Minerals and the Menstrual Cycle: Impacts on Ovulation and Endometrial Health
by
 , , ,
, , ,
Celine Kapper
1,
Peter Oppelt
1,2,
Clara Ganhör
3,4,
Ayberk Alp Gyunesh
1,
Barbara Arbeithuber
1,
Patrick Stelzl
2 and
Marlene Rezk-Füreder
1,* 1
Experimental Gynaecology, Obstetrics and Gynaecological Endocrinology, Johannes Kepler University Linz, Altenberger Strasse 69, 4040 Linz, Austria
2
Department for Gynaecology, Obstetrics and Gynaecological Endocrinology, Kepler University Hospital, Johannes Kepler University Linz, 4020 Linz, Austria
3
Division of Pathophysiology, Institute of Physiology and Pathophysiology, Medical Faculty, Johannes Kepler University Linz, 4020 Linz, Austria
4
Clinical Research Institute for Cardiovascular and Metabolic Diseases, Medical Faculty, Johannes Kepler University Linz, 4020 Linz, Austria
*
Author to whom correspondence should be addressed.
Nutrients 2024, 16(7), 1008; https://doi.org/10.3390/nu16071008
Submission received: 26 February 2024
/
Revised: 27 March 2024
/
Accepted: 28 March 2024
/
Published: 29 March 2024
(This article belongs to the Special Issue The Role of Nutrition in Gynecological Diseases)
Abstract
:The role of minerals in female fertility, particularly in relation to the menstrual cycle, presents a complex area of study that underscores the interplay between nutrition and reproductive health. This narrative review aims to elucidate the impacts of minerals on key aspects of the reproductive system: hormonal regulation, ovarian function and ovulation, endometrial health, and oxidative stress. Despite the attention given to specific micronutrients in relation to reproductive disorders, there is a noticeable absence of a comprehensive review focusing on the impact of minerals throughout the menstrual cycle on female fertility. This narrative review aims to address this gap by examining the influence of minerals on reproductive health. Each mineral’s contribution is explored in detail to provide a clearer picture of its importance in supporting female fertility. This comprehensive analysis not only enhances our knowledge of reproductive health but also offers clinicians valuable insights into potential therapeutic strategies and the recommended intake of minerals to promote female reproductive well-being, considering the menstrual cycle. This review stands as the first to offer such a detailed examination of minerals in the context of the menstrual cycle, aiming to elevate the understanding of their critical role in female fertility and reproductive health.
1. Introduction
Lifestyle factors such as weight, stress, smoking, and alcohol consumption can also significantly influence conception and the menstrual cycle [1,2,3]. This modern lifestyle, characterized by altered dietary habits, exposure to environmental pollutants, and increased stress, profoundly impacts an individual’s mineral status [4,5]. The exposure to heavy metals like lead and cadmium can antagonize mineral absorption and function, potentially worsening fertility challenges [6]. While the influence of minerals on male fertility has been intensively investigated [7,8,9,10], their role in women’s reproductive health and menstrual cycle has been marginally addressed, often only in the context of specific reproductive pathologies [11,12], emphasizing vitamins and multivitamin supplementation. Notably, these studies frequently lack in-depth investigation of the role of minerals and the underlying mechanisms, neglecting the phases of the menstrual cycle [13]. This review aims to address these gaps. We focus on individual minerals and their distinct roles in hormonal regulation, ovulation, oxidative stress, and endometrium health throughout the menstrual cycle. It provides a comprehensive overview of the role of minerals in female fertility and gives insights into potential therapeutic approaches for fertility challenges by offering evidence-based recommendations for mineral intake in reproductive-age women.
2. Hormonal Regulation and Fertility
2.1. Overview of Hormones and Fertility
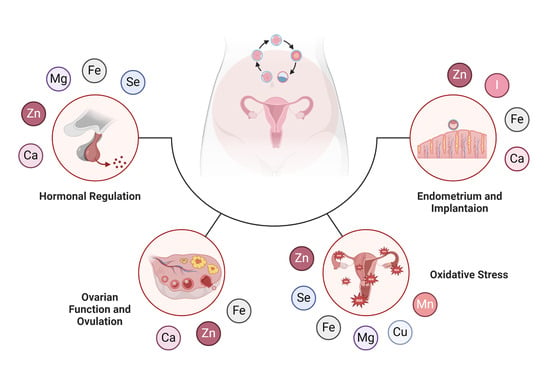
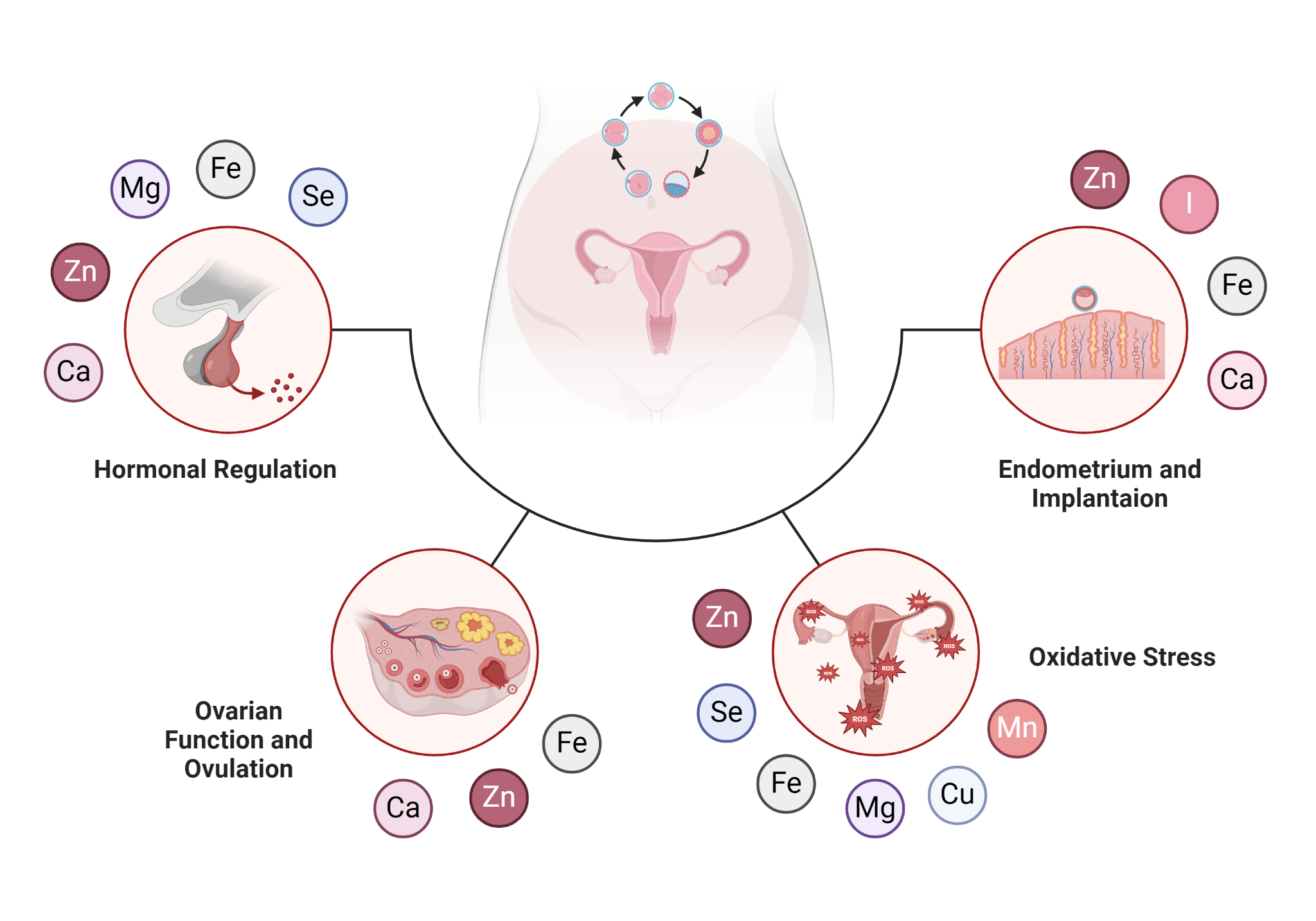
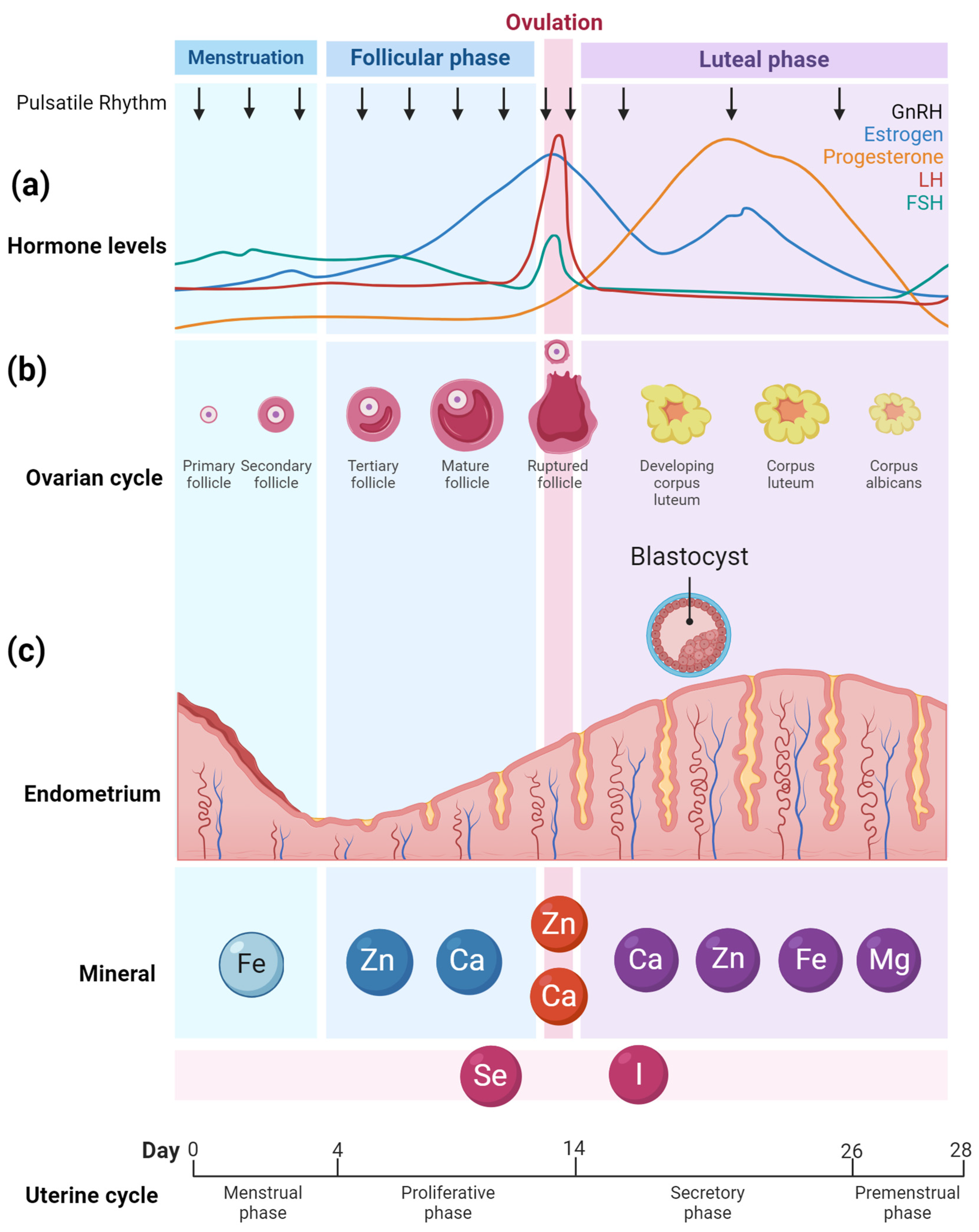
Human reproduction is regulated by hormones, guiding processes from the onset of menstrual cycles during puberty to the complexity of ovulation, implantation, and gestation [14]. At the cycle’s outset, declining estrogen and progesterone levels result in the elimination of the endometrial lining. As the follicular phase progresses, Follicle-Stimulating Hormone (FSH) promotes ovarian follicle growth, leading to an estrogen increase which suppresses FSH production. A Luteinizing Hormone (LH) increase, stimulated by peak estrogen levels, marks ovulation and the release of a mature egg. Post-ovulation, in the luteal phase, the transformed follicle—now the corpus luteum [15]—secretes progesterone and some estrogen, readying the endometrial lining for potential implantation [16]. FSH and LH are essential in this reproductive process. They regulate follicle maturation and ovulation, while estrogen and progesterone, produced by the follicles and corpus luteum, prime the endometrium for optimized conditions for a fertilized egg [17] (Figure 1a). While insulin is predominantly recognized for its role in regulating glucose metabolism, it also plays a crucial role in reproductive processes.
Iron (Fe) is essential for the menstrual cycle [18,19,20], with deficiencies causing hormonal imbalances [21,22,23,24,25] and anemia that affect blood flow to the ovaries and ovulation regularity [26,27,28]. During the follicular phase and ovulation, selenium (Se), calcium (Ca), and zinc (Zn) play pivotal roles. Ca is integral to gonadotropin-releasing hormone (GnRH) regulation [29,30], oocyte activation, and zygotic development [31,32], and it also modulates second messengers vital for sperm fusion [33,34,35]. During the first half of the menstrual cycle, known as the follicular phase, increased GnRH secretion stimulates the release of FSH and LH, which are crucial for follicle development and preparing the body for ovulation; in the second half, the luteal phase, GnRH secretion is reduced as rising progesterone levels from the corpus luteum exert negative feedback on the hypothalamus and pituitary gland [36]. Zn aids hormone synthesis [37] by influencing LH, FSH [38], and steroid synthesis [39,40], and, along with Se [41,42], safeguards the oocyte from reactive oxygen species (ROS) damage [43,44]. In the luteal phase, Ca [45,46], Zn [47,48], Fe [49,50,51,52,53], and magnesium (Mg) [54,55] collectively support endometrial function [56]. Ca, deposited at the embryo implantation site, controls endometrial receptivity [45,46]. Deficiencies in Fe [49,50,51,52,53] and zinc can impair this receptivity and hinder embryo implantation [47,48]. Mg, by relaxing smooth muscle [54], may influence retrograde menstruation [54,55] and reduce vascular endothelial growth factor, offering potential benefits for conditions like endometriosis [57,58,59]. Both iodine (I) and Se [60,61], due to their ties with thyroid hormones, are vital throughout the menstrual cycle [62]. Their deficiencies can disrupt hormonal balance [63], endometrial health [64], follicle development [65], and overall fertility [65,66]. Adapted from “Ovarian hormones throughout the menstrual cycle”, by BioRender.com (accessed on 27 March 2024).
Elevated levels of insulin can prompt the ovaries to produce increased androgens, such as testosterone, potentially interfering with processes governed by estrogen and progesterone [67,68]. Thus, balanced insulin levels are pivotal for both metabolic and reproductive efficiency [69]. Imbalances in insulin levels, as observed in conditions like polycystic ovary syndrome (PCOS), can disrupt hormonal pathways [14,70]. PCOS is a multifactorial endocrine disorder characterized by ovarian dysfunction, hyperandrogenism, and metabolic disturbances, with implications for reproductive, metabolic, and cardiovascular health [71].
2.2. Influence of Minerals on Hormonal Regulation
2.2.1. Zinc
Zinc (Zn) plays a multifaceted role in our body, particularly in hormonal activities. Not only is it vital for insulin metabolism [72], but also in testosterone synthesis [39,40,73]. Zinc finger proteins are involved in the genetic expression of steroid hormone receptors. Therefore, zinc plays a pivotal role in the expression of various hormonal activities, including the action of the metabolism of androgen hormones, estrogen, and progesterone [74,75,76].
For women, maintaining a balance of sex hormones is crucial: Any imbalances could result in reproductive issues [77,78,79]. The risk of preterm delivery was increased with low zinc intake (< or =6 mg/day) [77]. Testosterone, synthesized in the ovaries’ theca cells, is essential for follicle maturation [40]. A balance between the different sex hormones is necessary for the proper functioning of the menstrual cycle and follicle maturation [80,81]. Testosterone plays a key role in the regulation of female libido. A deficiency of testosterone can lead to reduced sexual desire [80]. Additionally, zinc interacts with steroid hormones [82] and is imperative for the proper functioning of estrogen receptors [83,84], which play a central role in the menstrual cycle [85,86] and overall female reproductive health [40,87,88]. Research has also underscored the involvement of zinc in follicular development [89,90,91,92,93] and ovulation [94,95,96]. Consequently, maintaining optimal zinc levels may be crucial for women aiming to optimize their fertility, especially at the time of the follicular phase and ovulation (Figure 1a) [75,97].
Throughout the menstrual cycle, serum zinc concentrations vary. According to a study by Michos C. et al., plasma zinc levels changed significantly between all times of the menstrual cycle. The highest levels were observed during ovulation and the lowest at the time of menstruation [76]. However, there is no clear relationship between serum zinc concentrations and infertility, but it highlights the importance of zinc for proper menstrual cycle function [37,98,99,100].
A zinc deficiency (<56 μg/dL) [78] can have adverse effects on women’s reproductive health. It might lead to issues like the altered synthesis or secretion of FSH and LH, irregular ovarian development, menstrual cycle disturbances, asynchronous uterine contractions, and even conditions like pre-eclampsia [37,38].
Research also hints at a potential link between zinc deficiency and PCOS pathogenesis, especially concerning insulin resistance [101] and testosterone levels [101,102]. Insulin resistance is a pronounced characteristic in many women with PCOS, and mean serum zinc levels were also significantly lower in PCOS women [101,103]. Investigations have demonstrated that zinc can enhance insulin sensitivity by acting as a cofactor for several enzymes engaged in carbohydrate metabolism [104]. Furthermore, zinc supplementation with 30 mg or 40 mg of zinc sulfate can optimize insulin secretion and its receptor binding [105], leading to improved glucose uptake and utilization [106].
2.2.2. Selenium
Selenium is essential for the production of selenoproteins, which are crucial for the conversion of the thyroid hormone thyroxine (T4) into its active form, triiodothyronine (T3) [60,63]. The proper transformation of T4 to T3 is central for regulating metabolic rate and numerous cellular processes within the body [61,64,107,108,109]. Proper thyroid function is crucial for a balanced hormonal environment in the female reproductive system [110]. Conditions like hyperthyroidism or hypothyroidism can disrupt the menstrual cycle [111,112], increase follicular atresia [113], lead to anovulation [114], and lead to impaired fertility [115,116,117]. Thyroid hormones both directly and indirectly modulate other essential reproductive hormones, such as progesterone and estrogen [63,115,118]. Ensuring optimal selenium levels might help manage the impact and severity of thyroid-related conditions, thereby influencing female reproductive health.
For optimal hormone regulation and consistent menstruation without anovulation, selenium is especially vital during the follicular phase, around ovulation, and throughout menstruation. Furthermore, the importance of selenium is not limited to the earlier phases, as it also has a crucial role in the luteal phase. Research conducted by Zagrodzki P. et al. [119,120] explored the interplay between selenium status, secretion of sex hormones, and thyroid metabolism in both adolescent girls and adult women. Their findings underscore a clear association between selenium levels and the female reproductive system, with particular emphasis on how selenium influences thyroid physiology in adolescent girls and young women during the luteal phase [119,120].
2.2.3. Iodine
Iodine is predominantly recognized for its pivotal role in thyroid function and plays a crucial role in the synthesis of thyroid hormones [121]. As mentioned above, these hormones interplay with reproductive hormones, such as progesterone and estrogen [115]. Thus, an imbalance due to either a deficiency or an excess of iodine can set off a cascade of effects, leading to disruptions in reproductive hormones. Such hormonal disruptions can hinder ovulation and compromise overall reproductive health, highlighting the subtle yet significant influence of iodine on fertility dynamics [62,66,121,122,123,124].
Iodine deficiency is one of the most common causes of hypothyroidism worldwide [125]. Iodine deficiency (iodine–creatinine ratios below 50 μg/g) in women is directly related to infertility, as reported by Mills and colleagues [123]. Hypothyroidism due to iodine deficiency in women results in significant reproductive changes, including anovulation [65] and decreased fertility [66], and when pregnancy occurs, gestational hypertension, stillbirths, and congenital anomalies, as well as increased perinatal mortality, may be observed [126,127,128]. A decline in thyroid function is associated with diminished blood-binding capacity for sex hormone-binding globulin (SHBG) [129]. SHBG plays a pivotal role in sequestering and transporting gonadal hormones in the circulatory system [130]. As a corollary of this diminished binding capacity, there is a noted decrease in the total concentrations of testosterone and estradiol, a primary estrogen [131]. Concurrently, there is an uptick in the fraction of these hormones that remain unbound to proteins [132]. Additionally, hypothyroidism can attenuate the response to LH [129], imperative for ovulation [133]. This attenuation can subsequently stimulate the secretion of thyrotropin-releasing hormone (TRH) [134]. An elevated concentration of this hormone can induce a surge in serum prolactin levels [135]. Elevated prolactin can disturb the consistent secretion of gonadotropin-releasing hormone (GnRH) [118], a critical regulator for the onset of the menstrual cycle and ovulation [136,137]. Such perturbations can manifest as ovulatory dysfunctions [138,139].
Due to the direct relationship between iodine and thyroid physiology, adequate iodine intake, just like selenium, must be maintained throughout the menstrual cycle (Figure 1a).
2.2.4. Iron
Iron is an essential component of hemoglobin, the protein in red blood cells that carries oxygen throughout the body [140]. Adequate oxygen transport is necessary for many bodily functions, including the function of the ovaries and uterus [18,140]. Beyond its function in oxygen transport, iron is essential to the operation of certain enzymes. These enzymes affect multiple biochemical pathways, including those related to hormone synthesis and regulation [18,19,20]; estrogen and iron metabolism in particular are closely related [141,142]. For instance, the Cytochrome-P450 enzymes, which process steroid hormones like estrogen and progesterone, significantly depend on iron [143]. Similarly, iron is indispensable for the enzymes Prolyl Hydroxylase [144] and Lysyl Hydroxylase [145] involved in collagen synthesis [146], thereby influencing the health of the connective tissue in reproductive organs [147]. As a consequence, an iron deficiency, often manifested as anemia, can lead to disturbances in menstrual cycles. Hormonal imbalances from such deficiencies can not only affect the regularity of the menstrual cycle but also reduce fertility potential [21,22,23,24,25].
2.2.5. Calcium
Calcium is renowned primarily for its role in bone health [148,149], but it also plays a significant role in the secretion and action of hormones [150], particularly in the synthesis and secretion of neurotransmitters [151]. These neurotransmitters influence the release of GnRH. The activity of GnRH neurons, especially their “burst-firing” mode, is affected by calcium ions [152]. This burst-firing activity is closely linked to the release of GnRH, a key hormone that controls the female menstrual cycle [153,154]. By stimulating the anterior pituitary gland, GnRH prompts the release of LH and FSH, which subsequently induce the ovaries to produce and release estrogen and progesterone. Disruptions in GnRH release can affect ovulation and thereby influence female fertility [29,30,151,152,155,156]. Additionally, calcium is involved in the release of insulin from the pancreas, highlighting its indirect role in metabolic pathways associated with hormonal regulation [14,157,158,159,160]. Calcium plays an important role, particularly during the ovulatory phase, as it influences the release of gonadotropin-releasing hormone (GnRH), which controls ovulation by stimulating the release of LH.
2.2.6. Magnesium
Magnesium is an essential mineral that plays a central role in hormonal regulation in the body, thereby also influencing female fertility [161]. It serves as a cofactor for a variety of enzymatic reactions, including those directly linked to the production and function of reproductive hormones. For instance, magnesium is involved in the activity of enzymes such as aromatase [162,163], responsible for converting androgens into estrogens [164].
Disruptions in these hormonal harmonies, as seen in conditions like PCOS, can spell challenges for fertility [165,166,167,168,169,170,171,172,173,174,175]. Through these mechanisms, adequate magnesium levels contribute to optimizing insulin sensitivity and stabilizing glucose metabolism. Research indicates that women with PCOS often exhibit lower serum magnesium levels compared to those without the condition [165,166,167,168,169,170,171,173,174]. Consequently, magnesium supplementation may represent a promising therapeutic avenue for PCOS patients to ameliorate insulin metabolism and reduce the risk of associated comorbidities [161,176,177,178,179,180]. While current research is not clear about the specific phase of the menstrual cycle where magnesium has the strongest influence on hormones, it is consistently emphasized that maintaining adequate magnesium levels throughout the cycle is crucial.
3. Ovarian Function and Ovulation
3.1. Overview of Ovarian Function
The ovaries, paired almond-sized organs located on each side of the uterus, play a central role in female reproductive health. Their primary functions include the production of oocytes for fertilization and the synthesis of key hormones, primarily estrogen and progesterone, which regulate menstrual cycles and support pregnancy [102,181,182,183,184,185,186,187].
The life of an oocyte begins with a primary follicle growing into a mature follicle (Figure 1b) and ends in the fetal period. Female fetuses have approximately 6–7 million potential follicles; however, by puberty, only about 400,000 remain [188,189]. Each menstrual cycle then witnesses a cohort of these follicles initiating development, though usually only one reaches full maturity and undergoes ovulation [190].
3.2. Influence of Minerals on Ovulation
3.2.1. Calcium
Calcium plays an important role in ovarian function and the progression of the female reproductive system [191,192,193]. Within the ovary, calcium influences follicular development and oocyte maturation (as in Figure 1b) [194,195,196]. It is instrumental in the intracellular signaling pathways that govern ovulation, facilitating the release of the oocyte from the follicle. Some of these crucial intracellular signaling pathways include the Store-Operated Calcium Entry (SOCE) [197], the Calcium/Calmodulin-dependent Protein Kinase II (CaMKII) pathway [198], and the Phospholipase C (PLC) pathway [199]. Additionally, calcium is indispensable during fertilization, participating in oocyte activation and the initiation of zygotic development [31,32]. Specifically, during these stages, calcium ions modulate the release of vital secondary messengers, including inositol trisphosphate (IP3) [33], cyclic adenosine monophosphate (cAMP) [34], and diacylglycerol (DAG) [35], which are essential for oocyte activation and its fusion with the spermatozoon [31,32]. In the early stages of embryonic development, a balanced calcium concentration is crucial for proper cellular division and the implantation of the embryo into the uterine lining [31,200,201,202,203]. Consequently, an imbalance in calcium levels, whether due to a deficiency [204,205] or excess [206], can compromise fertility and reduce the likelihood of a successful pregnancy [207]. Thus, for women aiming to conceive, it is crucial to maintain optimal calcium homeostasis to ensure the most conducive environment for fertilization and embryonic progression. In summary, calcium is particularly important during the phases of follicular development, egg maturation, ovulation, and fertilization in the female reproductive cycle.
3.2.2. Zinc
Zinc plays an integral role in oocyte maturation, quality, and functionality, serving as a pivotal element in various cellular and metabolic pathways crucial for the oocyte’s proper development and maturation [208,209]. It acts as a crucial cofactor for enzymes like DNA polymerase [210], ribonucleotide reductase [211], and thymidylate synthase [212], vital for DNA synthesis and repair [213,214]. Moreover, zinc influences cell cycle regulators such as zinc finger proteins [215] and the p53 protein [216], contributing to cell cycle regulation and cellular protection [37,93,217]. Numerous scientific investigations have highlighted that zinc deficiency can significantly perturb follicular development, a critical process wherein the oocyte matures within a protective sac of granulosa cells [88,94,218]. Disruptions in this complicated process, due to a zinc deficiency (Tian and Diaz 2013), can lead to ovulation disorders, which are characterized by impaired follicle rupture or impaired egg release [219]. Consequently, this diminishes the potential for successful fertilization and implantation [220,221,222].
Furthermore, zinc insufficiency can compromise oocyte quality [223], further attenuating its capacity for fertilization and subsequent embryonic development [91,224,225,226,227] potential for oocyte growth [228]. A deficiency in zinc triggers apoptosis that restricts the proliferation of cumulus cells [229]. These cells are vital for oocyte maturation, aiding in cytoplasmic maturation and growth by synthesizing glutathione (GSH) and delivering it to the oocytes. Thus, the suboptimal growth and development of cumulus cells detrimentally affect oocyte maturation and quality [230].
3.2.3. Iron
Iron, an indispensable trace element in the human body, plays a pivotal role in various physiological processes, including oxygen transport via hemoglobin in the bloodstream [231]. The ovaries, as specialized reproductive organs, rely heavily on a consistent and adequate oxygen supply to ensure the proper maturation of oocytes, which are crucial for successful fertilization and subsequent embryo development [232,233,234,235,236]. Iron’s involvement in DNA synthesis is important for the rapid cellular division observed during oocyte maturation and early embryonic stages [237]. Furthermore, iron is essential for mitochondrial function, ensuring that cells, including those in the ovaries, have the necessary energy for their intricate processes [235,238]. A deficiency in iron can lead to anemia, which may compromise the blood flow to the ovaries, potentially affecting the quality of oocytes and the regularity of ovulation [26,27,28]. This can have downstream effects on overall fertility, making the maintenance of optimal iron levels paramount for women wishing to conceive. A case–control study by Holzer et al. [239] in 2023 demonstrated an association between low ferritin levels—a substance with which cells can store iron—and unexplained infertility [239]. Thus, ensuring appropriate iron levels is not only vital for general health but is also intricately linked to female reproductive success. There has also been a significant association between iron overdose and lower egg counts noted in assisted reproductive technologies (ART) studies [53,240].
Two studies, one from 2022 [241] and one from 2023 [242], with 6551 participants suggest an association between changes in iron metabolism, particularly elevated ferritin levels, and ovarian endometriosis. Endometriosis is a chronic condition characterized by the presence of endometrial-like tissue outside the uterine cavity [243,244] leading to a microenvironment established by endometriotic lesions, which is dominated by inflammation and oxidative processes [245]. Ferritin and iron levels were found to be higher in cyst fluid than in serum, suggesting local iron accumulation [246]. The risk for endometriosis appears to increase with ferritin and transferrin levels up to a certain threshold, after which it stagnates [241,242,246]. However, further research is needed to clarify the exact role of iron metabolism in endometriosis.
4. Oxidative Stress and Fertility
4.1. Overview of Oxidative Stress and Its Influence on Fertility
Oxidative stress refers to an imbalance between the production of free radicals and the body’s ability to counteract or detoxify their harmful effects using antioxidants [247,248]. Free radicals, primarily reactive oxygen species (ROS), can cause damage to cellular structures, including DNA, proteins, and lipids [247,248].
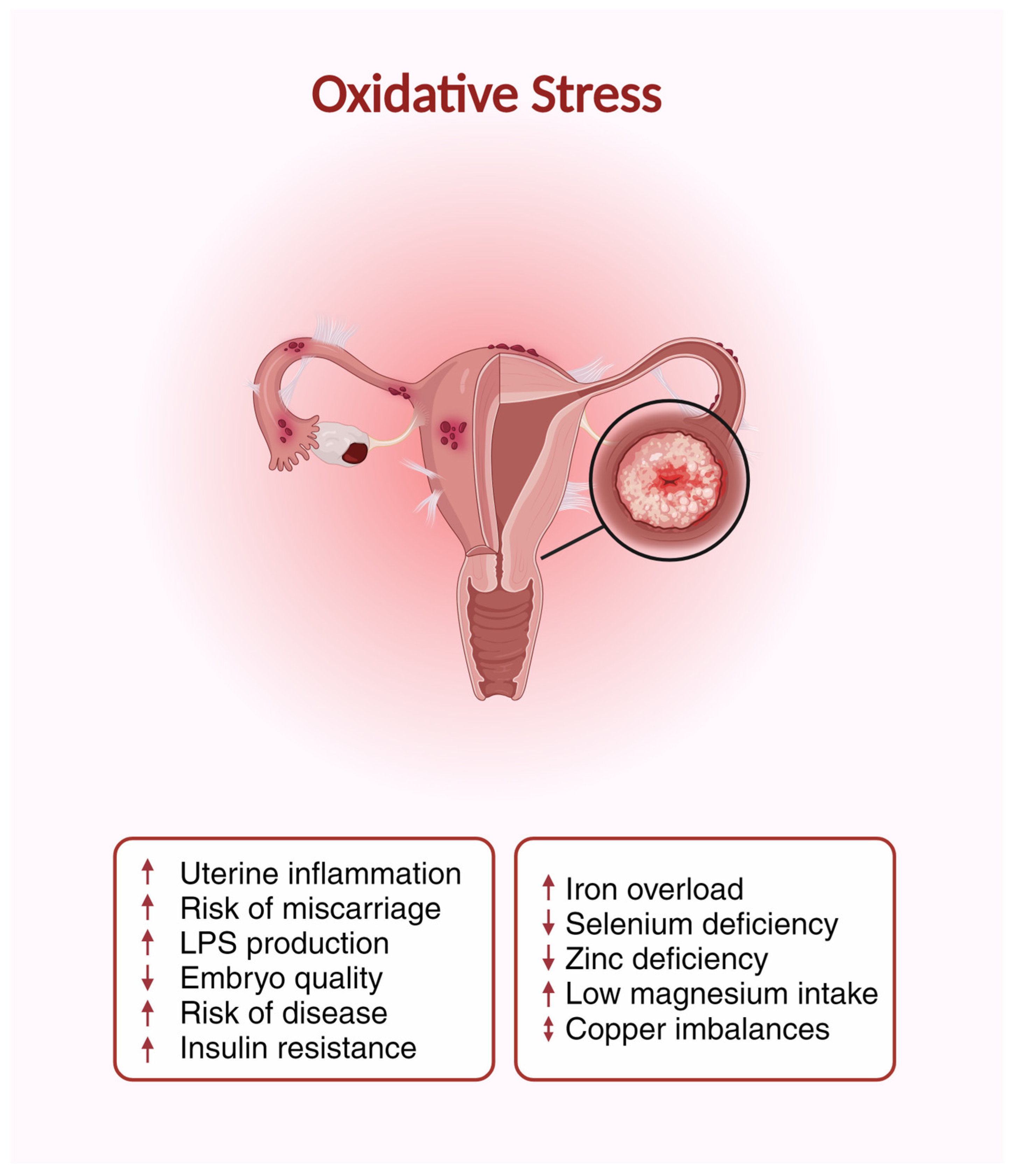
In the context of reproductive health, oxidative stress has been shown to play a pivotal role. Elevated ROS levels can impact the quality of both sperm [249] and oocytes [250], compromising their function and potentially reducing the chances of fertilization [251]. For instance, excessive ROS can cause DNA fragmentation in spermatozoa [252], diminishing its fertilizing potential. Likewise, oxidative stress in the ovarian microenvironment can impact the maturation, quality, and function of oocytes [183,251,252]. Moreover, post-fertilization, excessive ROS can hinder embryo development and implantation [253]. Diseases that cause infertility, such as endometriosis [254] and PCOS [255], have also been shown to have increased ROS levels. Minerals play a crucial role in the body’s defense mechanism against oxidative stress [256] (Figure 2). Their participation in enzymatic antioxidant systems aids in neutralizing the adverse effects of ROS [257].
Oxidative stress plays a central role in impairing female fertility [183]. Direct effects include increased uterine inflammation [258], increased risk of miscarriage [259], decreased embryo quality [43,183], increased risk of disease associated with reproduction [245,258,260], and growing insulin resistance that potentially impairs fertility [261]. Iron overload [262], deficiency of selenium [263], zinc deficiency [264], low magnesium intake [265], and imbalance of copper [266] in the body promote oxidative stress and, thus, have indirect effects on fertility. LPS (lipopolysaccharide) is a component of the outer membrane of Gram-negative bacteria that can promote oxidative stress, which impairs female fertility by increasing inflammation and damaging egg cells [267]. This illustration was created using BioRender.
4.2. Influence of Minerals on Oxidative Stress
4.2.1. Zinc
Zinc has remarkable antioxidant properties that make it an essential component in protecting the body from oxidative stress [106,264,268]. Zinc serves as a cofactor for various antioxidant enzymes, including superoxide dismutase (SOD) [268]. SOD facilitates the conversion of superoxide radicals into less harmful molecules, thus mitigating oxidative damage. Research has emphasized the importance of zinc in maintaining the optimal activity of SOD, offering protection against oxidative stress-induced damage in the reproductive system [37,209,269,270,271]. In the context of female fertility, zinc’s antioxidative function plays a pivotal role. It safeguards the oocytes, which are especially vulnerable to ROS-induced damage during maturation, thereby enhancing the likelihood of successful fertilization [99,272,273]. Concurrently, zinc facilitates the ovulation process by maintaining an ROS balance, promoting a consistent ovulatory cycle [43,219]. Post-fertilization, zinc serves a protective role for the developing embryo against ROS-induced harm, augmenting the prospects for successful implantation and development [44,274,275,276,277]. Therefore, an optimal zinc status can significantly augment a woman’s ability to produce healthy oocytes, ovulate successfully, and ultimately experience a successful pregnancy [209,221,278]. A deficiency in zinc can exacerbate health complications across various diseases, compromise immune functionality [279], and augment oxidative stress [280]. Despite limited research linking zinc to endometriosis, evidence suggests diminished zinc levels in afflicted women. This is particularly evident in the follicular fluid of the ovaries when compared to women with fallopian tube-related infertility [48,281]. Furthermore, zinc possesses anti-inflammatory attributes that might modulate the inflammatory processes so commonly observed in endometriosis, potentially increasing infertility [59,282,283]. However, proper dosing is essential since excessive zinc, though essential for myriad physiological processes, can exhibit pro-oxidative effects [279,284,285,286].
4.2.2. Selenium
While the association between selenium status and reproductive function is well-established in males [287,288], its elucidation in females remains an active area of investigation. Selenium plays an important role in protecting against oxidative damage, especially concerning fertility [41,263]. Optimal selenium concentrations are associated with enhanced fertility outcomes, attributable to the mitigation of oxidative stress in reproductive tissues [289,290,291].
Selenium’s antioxidative properties are integral to reproductive health [42]. Selenium is crucial to the function of the antioxidant enzyme glutathione peroxidase (GPx). GPx neutralizes hydrogen peroxide, a potent ROS, by converting it to water, preventing lipid peroxidation and potential damage to cellular membranes [292,293]. Oxidative stress, stemming from an excessive presence of free radicals, can adversely affect the ovulatory process [42,248,294]. This encompasses damage to ovarian follicles, compromised oocyte quality, and perturbations in the intricate hormonal equilibrium required for ovulation [295,296]. Selenium acts as a cofactor for a gamut of antioxidant enzymes, notably glutathione peroxidases, which counteract free radicals, attenuating the repercussions of oxidative stress on the ovaries [297,298,299,300]. Numerous studies emphasize the importance of maintaining optimal selenium levels to protect the ovaries from oxidative damage, thus ensuring a stable and efficient ovulation process [298,301]. In patients with endometriosis, a combined intake of vitamin E, C, selenium, and zinc was inversely correlated with disease severity [302]. A lower consumption of these antioxidants was associated with an increased intensity of the disease, suggesting a potential link between disease progression and the state of lipid peroxidation [59,302,303].
4.2.3. Copper
Copper is also essential in the body’s defense against oxidative stress, primarily as a cofactor for the enzyme Superoxide Dismutase (Cu, Zn-SOD) [266]. Beyond this, copper also modulates other antioxidative systems and can influence signal transduction processes and gene expression [304,305,306,307]. Pertaining to female reproduction, copper’s antioxidative properties serve to protect oocytes from oxidative stress, which is vital for their integrity and function [307,308]. Additionally, copper supports endothelial function, crucial for optimal blood flow to the uterus and ovaries, thus positively influencing fertility [309,310,311,312,313]. Notably, copper can also manifest pro-oxidative properties when present in excessive amounts [313].
4.2.4. Iron
Iron, an essential trace element within the human body, plays a dual role in relation to oxidative stress and reproductive health. On one hand, it is crucial for oxygen transport and DNA synthesis. On the other hand, an excess of circulating non-transferrin-bound iron can increase the production of ROS, leading to oxidative stress [262,314,315].
However, conditions such as hereditary hemochromatosis, a genetic disorder, can lead to hyper-absorption and excessive deposition of iron within the body [316,317]. Similarly, indiscriminate iron supplementation without appropriate medical indication can elevate oxidative stress risk [318].
Additionally, the susceptibility of oocytes to oxidative stress intensifies with age, a phenomenon known as ovarian aging [319,320,321]. In this context, iron can paradoxically play both protective and detrimental roles [23,321,322]. While adequate iron levels, supplemented in cases of deficiency, can increase oocyte quality [22], an excess can diminish it, augmenting the risk of compromised fertility [25,53].
4.2.5. Magnesium
Magnesium serves as a cofactor for over 600 enzymatic reactions [325], including those involved in the repair of DNA damage [326] induced by oxidative stress [327]. It is also essential for the proper functioning of glutathione, a primary antioxidant in the body [328,329]. A sufficient magnesium status can mitigate the production of free radicals that pose harm to cellular structure [330,331,332]. Conversely, magnesium deficiency has been demonstrated to exacerbate oxidative stress [333]. The antioxidative properties of magnesium may indirectly bolster fertility [334] by safeguarding against oxidative stress, which can detrimentally affect reproductive health [161,335,336]. Through its antioxidative attributes [327,337], magnesium can preserve oocyte quality [251], modulate the ovulatory process [251,338], and contribute to the healthy functioning of the endometrium (Figure 2) [115,183,325,337,339,340].
Based on this information, magnesium plays a crucial role during the follicular phase, concerning the maturation and quality of oocytes and the ovulation process. Additionally, it is significant during the luteal phase in relation to the healthy functioning of the endometrium.
4.2.6. Manganese
Manganese, an essential trace element, holds a distinguished role as an antioxidant, primarily as a cofactor for the enzyme manganese superoxide dismutase (Mn-SOD), which is pivotal in protecting cellular structures against oxidative stress [341,342]. As mentioned before, in the context of female fertility, oxidative stress can adversely affect oocyte quality and function. It may also disrupt hormonal equilibrium and the reproductive cycle [343]. Therefore, manganese, through its antioxidative attributes, may play a protective role in female reproductive health and enhance female fertility [344,345]. However, manganese, while an antioxidant at physiological levels, can contribute to oxidative stress in surfeit [346]. Consequences of such pro-oxidative states range from the degradation of oocyte quality to perturbation in ovarian function [347,348,349].
5. Endometrium and Embryo Implantation
5.1. Overview of Implantation and Endometrium in Fertility
The uterus, enveloped by its specialized endometrial lining [350], is paramount for embryo implantation and subsequent gestation [351]. This muscular organ, in its entirety, goes through considerable dynamic changes across the menstrual cycle [352]. The endometrium, its inner lining, undergoes thickening, secretion, and shedding, all intricately timed and regulated by hormones [353,354]. In a successful conception cycle, the fertilized embryo finds a receptive endometrium, initiates implantation, and sets the stage for continued gestation [353,355].
Implantation is the process when the blastocyst, having completed multiple divisions after fertilization, attaches to the receptive endometrial lining [356] (Figure 1c). This process commences roughly a week after ovulation and is a highly coordinated interplay between the embryo and the maternal endometrium [357].
Upon reaching the uterine cavity, the blastocyst emerges from its protective shell, the zona pellucida, in a process termed ‘hatching’ [358]. The trophectoderm cells of the hatching blastocyst then initiate adhesion by recognizing specific molecules on the luminal surface of the endometrium. Subsequently, the blastocyst delves into the endometrial stroma, facilitated by the enzymes it secretes [359]. At the same time, the endometrium undergoes a transformation into a decidua, creating a nutrient-rich environment that nurtures the swiftly dividing embryo [360].
5.2. Influence of Minerals on Implantation and Endometrium
5.2.1. Iron
An iron deficiency can entail significant challenges for both the mother and the budding fetus [361,362]. Iron was investigated in relation to the endometrium. A study by Rodriguez-Diaz et al., 2023 has revealed that a deficiency in iron may impact endometrial conditions and its receptiveness, potentially decreasing the chances of successful embryo implantation [53]. Additional research also underscores the significance of iron balance within both the endometrium and the embryo, suggesting this balance plays a crucial role in the endometrium’s receptivity to an embryo and the subsequent implantation process [49,50,51,52,53]. There is promising research regarding Fractalkine (FKN) [363,364]. It has been found that FKN mitigates the negative impacts of iron deficiency on the receptivity-related genes and proteins in human endometrial carcinoma cells HEC-1A [363].
Overall, these results suggest that iron may play an important role in the development of endometrial receptivity and embryo implantation (Figure 1c). Therefore, a balanced iron metabolism could be crucial for a successful pregnancy.
5.2.2. Magnesium
Studies have demonstrated that in women with endometriosis, the fallopian tubes contract irregularly and spasmodically. Magnesium is known to relax smooth muscle, potentially influencing retrograde menstruation, which is considered a primary cause of endometriosis [54,55]. A study on rats by Hosgorler et al. suggests that magnesium can decrease the levels of vascular endothelial growth factor (VEGF) in uterine tissue, which may be beneficial in the treatment of gynecological conditions like endometriosis [57,58,59]. However, human studies on the use of magnesium in endometriosis are limited, necessitating further research.
5.2.3. Zinc
Zinc extends its physiological influence far beyond DNA synthesis [365]. In the intricate landscape of the endometrial lining, zinc emerges as a key regulator, governing cellular proliferation and differentiation [56,366]. These processes are essential for the cyclical endometrial shifts that form the foundation of menstrual cycles, with the maturation and shedding of the endometrial layer being tightly regulated events [37,47,367].
A study by Onuma et al., 2023 suggests that zinc deficiency may play a role in the development of endometrial cysts, a type of ovarian cancer [48]. Patients with endometrial cysts exhibited lower serum zinc levels compared to those with benign non-endometrial cysts. In experimental assays, zinc depletion from endometrial epithelial cells led to enhanced cell proliferation, indicating that zinc may have a potential inhibitory role in this growth [48]. Additionally, it was observed that zinc deficiency influenced specific gene expression alterations, which were neutralized upon the reintroduction of zinc [48,281,368]. These findings propose that zinc supplementation might serve as a potential therapeutic strategy to impede the development of such cysts.
5.2.4. Calcium
During pregnancy, the amount of calcium in the uterine endometrial tissue increases, and calcium deposits are made at the site where the embryo implants in the uterus. These are critical steps for the onset of pregnancy [45,369,370]. The hormone estrogen has been identified as a factor that increases the uptake of calcium in the body and influences the activity of specific genes [371,372] in the endometrium that are crucial for the initiation of pregnancy [45,369,370]. Among the significant genes related to uterine function and development is the Homeobox A10 (HOXA10) gene [373]. It plays a pivotal role in uterine development and function [374,375]. Alterations in the expression of HOXA10 have been associated with implantation failure [376]. Furthermore, the Leukemia Inhibitory Factor (LIF) is another crucial molecule linked to embryo development [377]. Overall, these results indicate that an adequate calcium level in the body is a requirement for the successful implantation of the embryo and the initiation of pregnancy [45,203,370,378].
The results of another study by Zhang et al. demonstrate that calcium, in the form of large-conductance calcium-activated potassium channels (BK(Ca) channels), is expressed in the human endometrium and plays a significant role in regulating endometrial receptivity and embryo implantation [46]. The expression of these channels varies throughout the menstrual cycle and influences the attachment of embryos to the endometrial lining, as well as the expression of factors crucial for endometrial receptivity [379]. Additionally, BK(Ca) channels regulate the activity of NF-κB, a transcription factor involved in inflammatory processes and cell proliferation, while also affecting calcium homeostasis in endometrial cells. These findings suggest that calcium serves as a crucial regulator of endometrial function, playing a pivotal role in successful embryo implantation and pregnancy. Disorders in calcium metabolism may consequently impact fertility and reproduction [46].
5.2.5. Iodine
While limited research has been conducted in humans, studies using animal models have provided insights into the relationship between iodine and fertility, particularly its effects on the endometrium. In cows with unexplained infertility (UI), treatment involving uterine infusions of Lugol’s iodine has been found to improve fertility. This improvement has been attributed to the bactericidal properties of iodine, which may aid in the restoration of damaged endometrial tissue. Other proposed mechanisms include alterations in uterine pH and enhanced uterine blood flow [380]. Similarly, the intrauterine infusion of Polyvinylpyrrolidone-Iodine (PVP-I) in dairy cows can induce transient uterine inflammation while promoting the regeneration of endometrial epithelial cells and improving fertility. This suggests that iodine, present in PVP-I, may potentially play a role in enhancing uterine lining and embryo implantation [381,382]. Rats treated with Lipiodol, a substance containing iodine, exhibited changes in the phenotype of dendritic cells in the endometrium [383]. These cells play a role in regulating the establishment and maintenance of implanted embryos. Iodine in Lipiodol may be responsible for these immunological changes, potentially enhancing embryo implantation [124]. The results of a randomized controlled trial study suggest that Lipiodol may be effective as a fertility treatment for women with unexplained infertility and endometriosis-related infertility [384]. The exact mechanism by which Lipiodol affects fertility is not yet fully understood, but it is thought that it may improve the receptivity of the endometrium to embryo implantation. While smaller doses of iodine appeared beneficial in creating a favorable uterine environment for reproduction in rats, the infusion of a large iodine dose into the uteri of mares resulted in severe tissue damage. This suggests that high doses of iodine can be toxic [124,385]. Adverse effects of maternal iodine excess were also shown by Sihan Wang et al. in 2023, and a negative effect on the neurological development and physical growth of infants was also shown during the early stages of pregnancy. In the study, it was shown that maternal serum iodine concentrations above 92 µg/L in the first trimester had adverse effects on infants’ development, while in the third trimester, levels above 92 µg/L positively influenced infants’ height. Suitable serum iodine concentration values in the first trimester ranged from 40 to 92 µg/L [386]. However, it is also noted that maternal iodine excess during the third trimester may have a positive impact on infant length growth [127,386,387]. Additionally, in a study of 501 women with moderate to severe iodine deficiency, pregnancy was delayed, and the likelihood of conception in each cycle decreased by 46% compared to non-iodine-deficient women [4,123,388].
6. Conclusions
In conclusion, based on this comprehensive review of the role of minerals in female fertility, it has become abundantly clear that each mineral examined—zinc, magnesium, calcium, iodine, selenium, iron, copper, and manganese—plays a significant role in the biological processes that underpin reproductive health. The interactions of these minerals with key determinants of fertility such as hormonal regulation, ovarian function, ovulation, oxidative stress, and endometrial implantation are complex and critical (Table 1).
Ensuring the optimal health of the female reproductive organs requires the careful regulation of mineral homeostasis, as zinc is essential for the modulation of insulin metabolism, steroidogenesis, and the control of ovulation cycles. It also protects the embryo from oxidative damage and supports endometrial cell proliferation. A zinc deficiency can manifest itself in impaired folliculogenesis [88,94,276] and menstrual irregularities [37], while an excess of zinc can increase pro-oxidative conditions and thus impair fertility [253,286].
Magnesium serves as a central cofactor in estrogenic metabolic pathways [389] and in glucose homeostasis [390], which is particularly important in people with polycystic ovary syndrome (PCOS) [391]. Hypomagnesemia can increase oxidative stress and impair oocyte viability [392] and endometrial functionality [183]. Normomagnesemia is generally maintained by renal regulatory mechanisms, so hypermagnesemia is less likely to be a problem [393].
Calcium, an important regulator of gonadotropin-releasing hormone (GnRH) secretion [394], is critical to the mechanisms of ovulation and embryo implantation [395]. Imbalances in calcium homeostasis—be it hypocalcemia or hypercalcemia—can hinder gametic [45,46] and zygotic development [31,32], emphasizing the need for balanced calcium intake during the follicular and ovulatory phases [191,395].
Iodine’s critical involvement in thyroxine synthesis and the consequent impact on reproductive hormones implicates its deficiency in anovulation and cyclical disturbances [65,66]. Excess iodine, particularly during the early stages of pregnancy [383,384,386], is associated with adverse developmental outcomes, necessitating prudent iodine management across the reproductive spectrum.
Selenium, embedded within the selenoprotein-dependent pathways of thyroid hormone conversion [60,61], is essential for ovarian protection and ovulatory integrity [41,42]. Selenium deficiency may lead to menstrual and ovulatory disruptions, whereas its excess can lead to toxicity [41,42].
Iron, which is central to endocrine synthesis and regulation, has an ambivalent impact on reproductive health. Iron deficiency can lead to menstrual abnormalities [21,22,23,24,25] and affect gamete cell quality [26,27,28], while iron excess is associated with inflammatory conditions such as endometriosis [241,242,246], emphasizing the need for careful iron monitoring.
Copper is beneficial as a crucial antioxidant cofactor [304,305,306,307] for oocyte maintenance [307,308], but excess copper can trigger oxidative stress, highlighting the need to avoid copper-induced reproductive toxicity.
Collectively, these insights underscore the imperative for clinicians to recommend mineral supplementation with precision, tailored to individual health profiles, dietary patterns, and reproductive aspirations, to foster optimal reproductive well-being.

{kind=link}
{kind=link}
{kind=link}
Table 1.
Impact of Minerals of Essential Minerals on Fertility. Zn, Mg, Ca, I, Se, Fe, Cu, and Mn on key determinants of female fertility: Hormonal Regulation, Ovarian Function, Ovulation, Oxidative Stress, and Endometrial Implantation.
Table 1.
Impact of Minerals of Essential Minerals on Fertility. Zn, Mg, Ca, I, Se, Fe, Cu, and Mn on key determinants of female fertility: Hormonal Regulation, Ovarian Function, Ovulation, Oxidative Stress, and Endometrial Implantation.
| Mineral | Hormonal Regulation | Ovarian Function and Ovulation | Oxidative Stress | Endometrium and Implantation |
|---|---|---|---|---|
| Zn | Insulin metabolism [105] Steroid synthesis [39,40] Hormone Balance [37] Regulation of LH and FSH [38] Ovulation [219] | Oocyte maturation [208,209], development [228], and quality [226] | Antioxidant properties [264,269], protect embryos from ROS [43,44], and modulate inflammation in endometriosis [281,368] | Cellular proliferation and differentiation in the endometrium [56], neutralizes alterations [279] and deficiency correlates with endometrial cysts and polyps [47,48] |
| Mg | Cofactor for the production and function of estrogen [163,164], stabilizing glucose metabolism [174] and disbalances are associated with PCOS [165,166,168] | Mg deficiency leads to oxidative stress [327,329,330]. Magnesium can preserve the quality of the oocyte [251,327], modulate the ovulation process [338], and contribute to the healthy functioning of the endometrium [337]. | Relax smooth muscle [54], influence retrograde menstruation [54,55], and reduce vascular endothelial growth factor, which may be beneficial in the treatment of gynecological conditions like endometriosis [57,58,59] | |
| Ca | Calcium influences the release of GnRH, and therefore the menstrual cycle [29,30] Necessary for ovulation [396] | Oocyte activation and zygotic development [31,32], oocyte activation and fusion with sperm [33,34,35] | - | Calcium is deposited at the site of embryo implantation and regulates endometrial receptivity and embryo implantation [45,46] |
| I | Thyroid function and the synthesis of thyroid hormones, also reproductive hormones [62]. Deficiency [397], resulting in anovulation, reduced fertility, and menstrual cycle disturbances [65,66] | - | - | Improving endometrial receptivity [380,381,382] and supporting embryo implantation through endometrial changes [383,384,386] |
| Se | Thyroid function and thus important for hormone regulation [60,61] Thyroid disorders can lead to disrupted menstrual cycles and anovulation [63,64] | - | Supporting Glutathione Peroxidase (GPx) [263,290,293] Efficient ovulation and protection of the ovaries from damage [41,42] | - |
| Fe | Hormone synthesis and regulation of estrogen and progesterone [18,19,20] Deficiency can cause hormonal imbalances and affect menstrual cycles [21,22,23,24,25] | Maturation of oocytes [232,233,234,235,236] and cellular division during oocyte maturation [237] Deficiency leads to anemia, compromises the blood flow to the ovaries, and affects the quality of oocytes and the regularity of ovulation [26,27,28] | Deficiency and overdose lead to oxidative stress [262,314,315] and both reduce oocyte quality [24,102,236,323] | Deficiency impacts endometrial conditions and its receptiveness and decreases embryo implantation [49,50,51,52,53] Ferritin overdose is in correlation with endometriosis [241,242,246] |
| Cu | - | Cofactor for Superoxide Dismutase [266] and modulates antioxidant systems [304,305,306,307] Protects oocytes from oxidative stress [307,308] and supports endothelial function; crucial for optimal blood flow to the uterus and ovaries [309,310,311,312,313] | - | |
| Mn | - | Cofactor for Superoxide Dismutase [341,342] and therefore supports oocyte quality and function [344,345] Overdose can contribute to oxidative stress and can damage oocyte and ovarian function [347,348,349] | - | |
Furthermore, the review provides actionable insights into appropriate mineral intake, offering guidelines for daily consumption based on different population groups—such as general women and pregnant women—and highlights the primary dietary sources for these minerals (Table 2). Such information is invaluable for clinicians who are tasked with advising women on how to optimize their reproductive health through nutrition.
In summary, the critical review and the data presented in Table 1 and Table 2 collectively contribute to a deeper understanding of mineral nutrition’s role in female fertility. They emphasize the importance of a balanced intake of essential minerals and provide a foundation for further research and clinical practice.
Author Contributions
Conceptualization, C.K. and M.R.-F.; methodology, C.K.; writing—original draft preparation, C.K.; writing—review and editing, C.K., P.O., C.G., A.A.G., B.A., P.S. and M.R.-F.; supervision, M.R.-F. All authors have read and agreed to the published version of the manuscript.
Funding
Open Access Funding by the University of Linz.
Acknowledgments
Supported by the Johannes Kepler Open Access Publishing Fund.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Chavarro, J.E.; Rich-Edwards, J.W.; Rosner, B.A.; Willett, W.C. Diet and Lifestyle in the Prevention of Ovulatory Disorder Infertility. Obstet. Gynecol. 2007, 110, 1050–1058. [Google Scholar] [CrossRef] [PubMed]
- Legro, R.S.; Chen, G.; Kunselman, A.R.; Schlaff, W.D.; Diamond, M.P.; Coutifaris, C.; Carson, S.A.; Steinkampf, M.P.; Carr, B.R.; McGovern, P.G.; et al. Smoking in Infertile Women with Polycystic Ovary Syndrome: Baseline Validation of Self-Report and Effects on Phenotype. Hum. Reprod. 2014, 29, 2680–2686. [Google Scholar] [CrossRef] [PubMed]
- Ethier, A.R.; McKinney, T.L.; Tottenham, L.S.; Gordon, J.L. The Effect of Reproductive Hormones on Women’s Daily Smoking across the Menstrual Cycle. Biol. Sex Differ. 2021, 12, 41. [Google Scholar] [CrossRef] [PubMed]
- Skoracka, K.; Ratajczak, A.E.; Rychter, A.M.; Dobrowolska, A.; Krela-Kaźmierczak, I. Female Fertility and the Nutritional Approach: The Most Essential Aspects. Adv. Nutr. 2021, 12, 2372–2386. [Google Scholar] [CrossRef] [PubMed]
- Gaskins, A.J.; Chavarro, J.E. Diet and Fertility: A Review. Am. J. Obstet. Gynecol. 2018, 218, 379–389. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Sharma, A. Cadmium Toxicity: Effects on Human Reproduction and Fertility. Rev. Environ. Health 2019, 34, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Mirnamniha, M.; Faroughi, F.; Tahmasbpour, E.; Ebrahimi, P.; Beigi Harchegani, A. An Overview on Role of Some Trace Elements in Human Reproductive Health, Sperm Function and Fertilization Process. Rev. Environ. Health 2019, 34, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Buhling, K.J.; Laakmann, E. The Effect of Micronutrient Supplements on Male Fertility. Curr. Opin. Obstet. Gynecol. 2014, 26, 199–209. [Google Scholar] [CrossRef]
- Almujaydil, M.S. The Role of Dietary Nutrients in Male Infertility: A Review. Life 2023, 13, 519. [Google Scholar] [CrossRef]
- Mora-Esteves, C.; Shin, D. Nutrient Supplementation: Improving Male Fertility Fourfold. Semin. Reprod. Med. 2013, 31, 293–300. [Google Scholar] [CrossRef]
- Dring, J.C.; Forma, A.; Chilimoniuk, Z.; Dobosz, M.; Teresiński, G.; Buszewicz, G.; Flieger, J.; Cywka, T.; Januszewski, J.; Baj, J. Essentiality of Trace Elements in Pregnancy, Fertility, and Gynecologic Cancers-A State-of-the-Art Review. Nutrients 2021, 14, 185. [Google Scholar] [CrossRef] [PubMed]
- Rezk, M.; Grasegger, L.; Brandstetter, N.; Pol-Edern, L.R.; Stelzl, P.; Oppelt, P.; Arbeithuber, B. Biomarker Screening in Preeclampsia: An RNA-Sequencing Approach Based on Data from Multiple Studies. J. Hypertens. 2022, 40, 2022–2036. [Google Scholar] [CrossRef] [PubMed]
- Grajecki, D.; Zyriax, B.-C.; Buhling, K.J. The Effect of Micronutrient Supplements on Female Fertility: A Systematic Review. Arch. Gynecol. Obstet. 2012, 285, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Herbison, A.E.; Porteous, R.; Pape, J.-R.; Mora, J.M.; Hurst, P.R. Gonadotropin-Releasing Hormone Neuron Requirements for Puberty, Ovulation, and Fertility. Endocrinology 2008, 149, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Hillier, S.G. Gonadotropic Control of Ovarian Follicular Growth and Development. Mol. Cell. Endocrinol. 2001, 179, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Richards, J.S.; Russell, D.L.; Ochsner, S.; Espey, L.L. Ovulation: New Dimensions and New Regulators of the Inflammatory-like Response. Annu. Rev. Physiol. 2002, 64, 69–92. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, J.; Ghosh, D. Role of Progesterone on Peri-Implantation Stage Endometrium-Embryo Interaction in the Primate. Steroids 2000, 65, 753–762. [Google Scholar] [CrossRef] [PubMed]
- Percy, L.; Mansour, D.; Fraser, I. Iron Deficiency and Iron Deficiency Anaemia in Women. Best Pract. Res. Clin. Obstet. Gynaecol. 2017, 40, 55–67. [Google Scholar] [CrossRef] [PubMed]
- Dutt, S.; Hamza, I.; Bartnikas, T.B. Molecular Mechanisms of Iron and Heme Metabolism. Annu. Rev. Nutr. 2022, 42, 311–335. [Google Scholar] [CrossRef]
- Srole, D.N.; Ganz, T. Erythroferrone Structure, Function, and Physiology: Iron Homeostasis and beyond. J. Cell. Physiol. 2021, 236, 4888–4901. [Google Scholar] [CrossRef]
- Peña-Rosas, J.P.; De-Regil, L.M.; Gomez Malave, H.; Flores-Urrutia, M.C.; Dowswell, T. Intermittent Oral Iron Supplementation during Pregnancy. Cochrane Database Syst. Rev. 2015, 2015, CD009997. [Google Scholar] [CrossRef] [PubMed]
- Petraglia, F.; Dolmans, M.M. Iron Deficiency Anemia: Impact on Women’s Reproductive Health. Fertil. Steril. 2022, 118, 605–606. [Google Scholar] [CrossRef]
- Mirza, F.G.; Abdul-Kadir, R.; Breymann, C.; Fraser, I.S.; Taher, A. Impact and Management of Iron Deficiency and Iron Deficiency Anemia in Women’s Health. Expert Rev. Hematol. 2018, 11, 727–736. [Google Scholar] [CrossRef] [PubMed]
- Cappellini, M.D.; Santini, V.; Braxs, C.; Shander, A. Iron Metabolism and Iron Deficiency Anemia in Women. Fertil. Steril. 2022, 118, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Ni, Z.; Li, Y.; Song, D.; Ding, J.; Mei, S.; Sun, S.; Cheng, W.; Yu, J.; Zhou, L.; Kuang, Y.; et al. Iron-Overloaded Follicular Fluid Increases the Risk of Endometriosis-Related Infertility by Triggering Granulosa Cell Ferroptosis and Oocyte Dysmaturity. Cell Death Dis. 2022, 13, 579. [Google Scholar] [CrossRef] [PubMed]
- Tonai, S.; Kawabata, A.; Nakanishi, T.; Lee, J.Y.; Okamoto, A.; Shimada, M.; Yamashita, Y. Iron Deficiency Induces Female Infertile in Order to Failure of Follicular Development in Mice. J. Reprod. Dev. 2020, 66, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Miller, E.M. The Reproductive Ecology of Iron in Women. Am. J. Phys. Anthropol. 2016, 159, S172–S195. [Google Scholar] [CrossRef] [PubMed]
- Osungbade, K.O.; Oladunjoye, A.O. Preventive Treatments of Iron Deficiency Anaemia in Pregnancy: A Review of Their Effectiveness and Implications for Health System Strengthening. J. Pregnancy 2012, 2012, 454601. [Google Scholar] [CrossRef] [PubMed]
- Constantin, S.; Jasoni, C.; Romanò, N.; Lee, K.; Herbison, A.E. Understanding Calcium Homeostasis in Postnatal Gonadotropin-Releasing Hormone Neurons Using Cell-Specific Pericam Transgenics. Cell Calcium 2012, 51, 267–276. [Google Scholar] [CrossRef]
- Herbison, A.E. Control of Puberty Onset and Fertility by Gonadotropin-Releasing Hormone Neurons. Nat. Rev. Endocrinol. 2016, 12, 452–466. [Google Scholar] [CrossRef]
- Webb, S.E.; Miller, A.L. Calcium Signalling during Embryonic Development. Nat. Rev. Mol. Cell Biol. 2003, 4, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, M. Calcium at Fertilization and in Early Development. Physiol. Rev. 2006, 86, 25–88. [Google Scholar] [CrossRef]
- Machaty, Z. Signal Transduction in Mammalian Oocytes during Fertilization. Cell Tissue Res. 2016, 363, 169–183. [Google Scholar] [CrossRef]
- Amireault, P.; Dubé, F. Intracellular cAMP and Calcium Signaling by Serotonin in Mouse Cumulus-Oocyte Complexes. Mol. Pharmacol. 2005, 68, 1678–1687. [Google Scholar] [CrossRef] [PubMed]
- Anifandis, G.; Michopoulos, A.; Daponte, A.; Chatzimeletiou, K.; Simopoulou, M.; Messini, C.I.; Polyzos, N.P.; Vassiou, K.; Dafopoulos, K.; Goulis, D.G. Artificial Oocyte Activation: Physiological, Pathophysiological and Ethical Aspects. Syst. Biol. Reprod. Med. 2019, 65, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Ortmann, O.; Weiss, J.M.; Diedrich, K. Gonadotrophin-Releasing Hormone (GnRH) and GnRH Agonists: Mechanisms of Action. Reprod. Biomed. Online 2002, 5 (Suppl. S1), 1–7. [Google Scholar] [CrossRef]
- Nasiadek, M.; Stragierowicz, J.; Klimczak, M.; Kilanowicz, A. The Role of Zinc in Selected Female Reproductive System Disorders. Nutrients 2020, 12, 2464. [Google Scholar] [CrossRef]
- Bedwal, R.S.; Bahuguna, A. Zinc, Copper and Selenium in Reproduction. Experientia 1994, 50, 626–640. [Google Scholar] [CrossRef]
- Baltaci, A.K.; Mogulkoc, R.; Baltaci, S.B. Review: The Role of Zinc in the Endocrine System. Pak. J. Pharm. Sci. 2019, 32, 231–239. [Google Scholar]
- Te, L.; Liu, J.; Ma, J.; Wang, S. Correlation between Serum Zinc and Testosterone: A Systematic Review. J. Trace Elem. Med. Biol. 2023, 76, 127124. [Google Scholar] [CrossRef]
- Lima, L.G.; Santos, A.A.M.D.; Gueiber, T.D.; Gomes, R.Z.; Martins, C.M.; Chaikoski, A.C. Relation between Selenium and Female Fertility: A Systematic Review. Rev. Bras. Ginecol. Obstet. 2022, 44, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Mistry, H.D.; Broughton Pipkin, F.; Redman, C.W.G.; Poston, L. Selenium in Reproductive Health. Am. J. Obstet. Gynecol. 2012, 206, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Camp, O.G.; Bembenek, J.N.; Goud, P.T.; Awonuga, A.O.; Abu-Soud, H.M. The Implications of Insufficient Zinc on the Generation of Oxidative Stress Leading to Decreased Oocyte Quality. Reprod. Sci. 2023, 30, 2069–2078. [Google Scholar] [CrossRef] [PubMed]
- Brion, L.P.; Heyne, R.; Lair, C.S. Role of Zinc in Neonatal Growth and Brain Growth: Review and Scoping Review. Pediatr. Res. 2021, 89, 1627–1640. [Google Scholar] [CrossRef] [PubMed]
- Tong, X.-M.; Lin, X.-N.; Song, T.; Liu, L.; Zhang, S.-Y. Calcium-Binding Protein S100P Is Highly Expressed during the Implantation Window in Human Endometrium. Fertil. Steril. 2010, 94, 1510–1518. [Google Scholar] [CrossRef]
- Zhang, R.-J.; Zou, L.-B.; Zhang, D.; Tan, Y.-J.; Wang, T.-T.; Liu, A.-X.; Qu, F.; Meng, Y.; Ding, G.-L.; Lu, Y.-C.; et al. Functional Expression of Large-Conductance Calcium-Activated Potassium Channels in Human Endometrium: A Novel Mechanism Involved in Endometrial Receptivity and Embryo Implantation. J. Clin. Endocrinol. Metab. 2012, 97, 543–553. [Google Scholar] [CrossRef]
- Yılmaz, B.K.; Evliyaoğlu, Ö.; Yorgancı, A.; Özyer, Ş.; Üstün, Y.E. Serum Concentrations of Heavy Metals in Women with Endometrial Polyps. J. Obstet. Gynaecol. 2020, 40, 541–545. [Google Scholar] [CrossRef] [PubMed]
- Onuma, T.; Mizutani, T.; Fujita, Y.; Ohgami, N.; Ohnuma, S.; Kato, M.; Yoshida, Y. Zinc Deficiency Is Associated with the Development of Ovarian Endometrial Cysts. Am. J. Cancer Res. 2023, 13, 1049–1066. [Google Scholar] [PubMed]
- Defrère, S.; Lousse, J.C.; González-Ramos, R.; Colette, S.; Donnez, J.; Van Langendonckt, A. Potential Involvement of Iron in the Pathogenesis of Peritoneal Endometriosis. Mol. Hum. Reprod. 2008, 14, 377–385. [Google Scholar] [CrossRef]
- Yao, Y.M.; Osuchowski, M.F.; Pan, Z.K.; Wang, J.H. Immune Dysfunction: An Update of New Immune Cell Subsets and Cytokines in Sepsis; Frontiers Media SA: Lausanne, Switzerland, 2022; ISBN 978-2-88-974248-6. [Google Scholar]
- Chavarro, J.E.; Rich-Edwards, J.W.; Rosner, B.A.; Willett, W.C. Iron Intake and Risk of Ovulatory Infertility. Obstet. Gynecol. 2006, 108, 1145–1152. [Google Scholar] [CrossRef]
- Li, Y.Q.; Cao, X.X.; Bai, B.; Zhang, J.N.; Wang, M.Q.; Zhang, Y.H. Severe Iron Deficiency Is Associated with a Reduced Conception Rate in Female Rats. Gynecol. Obstet. Investig. 2014, 77, 19–23. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Díaz, R.; Blanes-Zamora, R.; Paz-Montelongo, S.; Gómez-Rodríguez, J.; Fiestas, S.R.; González-Weller, D.; Gutiérrez, Á.J.; Rubio, C.; Hardisson, A.; Niebla-Canelo, D.; et al. The Influence of Follicular Fluid Metals on Assisted Reproduction Outcome. Biol. Trace Elem. Res. 2023, 201, 5069–5082. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, E.K.; Singer, H.A.; Rembold, C.M. Magnesium Relaxes Arterial Smooth Muscle by Decreasing Intracellular Ca2+ without Changing Intracellular Mg2+. J. Clin. Investig. 1992, 89, 1988–1994. [Google Scholar] [CrossRef] [PubMed]
- Mathias, J.R.; Franklin, R.; Quast, D.C.; Fraga, N.; Loftin, C.A.; Yates, L.; Harrison, V. Relation of Endometriosis and Neuromuscular Disease of the Gastrointestinal Tract: New Insights. Fertil. Steril. 1998, 70, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhou, W.; Miao, S.; Dong, X.; Zou, X. Effects of Zinc on Cell Proliferation, Zinc Transport, and Calcium Deposition in Primary Endometrial Epithelial Cells of Laying Hens In Vitro. Biol. Trace Elem. Res. 2021, 199, 4251–4259. [Google Scholar] [CrossRef] [PubMed]
- Hoşgörler, F.; Kızıldağ, S.; Ateş, M.; Argon, A.; Koç, B.; Kandis, S.; Güvendi, G.; Ilgin, R.; Uysal, N. The Chronic Use of Magnesium Decreases VEGF Levels in the Uterine Tissue in Rats. Biol. Trace Elem. Res. 2020, 196, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Harris, H.R.; Chavarro, J.E.; Malspeis, S.; Willett, W.C.; Missmer, S.A. Dairy-Food, Calcium, Magnesium, and Vitamin D Intake and Endometriosis: A Prospective Cohort Study. Am. J. Epidemiol. 2013, 177, 420–430. [Google Scholar] [CrossRef] [PubMed]
- Yalçın Bahat, P.; Ayhan, I.; Üreyen Özdemir, E.; İnceboz, Ü.; Oral, E. Dietary Supplements for Treatment of Endometriosis: A Review. Acta Biomed. 2022, 93, e2022159. [Google Scholar]
- Bhuyan, A.K.; Sarma, D.; Saikia, U.K. Selenium and the Thyroid: A Close-Knit Connection. Indian J. Endocrinol. Metab. 2012, 16, S354–S355. [Google Scholar] [CrossRef]
- Mojadadi, A.; Au, A.; Salah, W.; Witting, P.; Ahmad, G. Role for Selenium in Metabolic Homeostasis and Human Reproduction. Nutrients 2021, 13, 3256. [Google Scholar] [CrossRef]
- Harding, K.B.; Peña-Rosas, J.P.; Webster, A.C.; Yap, C.M.; Payne, B.A.; Ota, E.; De-Regil, L.M. Iodine Supplementation for Women during the Preconception, Pregnancy and Postpartum Period. Cochrane Database Syst. Rev. 2017, 3, CD011761. [Google Scholar] [CrossRef]
- Krassas, G.E.; Poppe, K.; Glinoer, D. Thyroid Function and Human Reproductive Health. Endocr. Rev. 2010, 31, 702–755. [Google Scholar] [CrossRef]
- Dosiou, C. Thyroid and Fertility: Recent Advances. Thyroid 2020, 30, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Medenica, S.; Nedeljkovic, O.; Radojevic, N.; Stojkovic, M.; Trbojevic, B.; Pajovic, B. Thyroid Dysfunction and Thyroid Autoimmunity in Euthyroid Women in Achieving Fertility. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 977–987. [Google Scholar] [PubMed]
- Ferri, N.; Ulisse, S.; Aghini-Lombardi, F.; Graziano, F.M.; Di Mattia, T.; Russo, F.P.; Arizzi, M.; Baldini, E.; Trimboli, P.; Attanasio, D.; et al. Iodine Supplementation Restores Fertility of Sheep Exposed to Iodine Deficiency. J. Endocrinol. Investig. 2003, 26, 1081–1087. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Papalou, O.; Kandaraki, E.A. The Role of Androgen Excess on Insulin Sensitivity in Women. Front. Horm. Res. 2019, 53, 50–64. [Google Scholar]
- Xu, Y.; Qiao, J. Association of Insulin Resistance and Elevated Androgen Levels with Polycystic Ovarian Syndrome (PCOS): A Review of Literature. J. Healthc. Eng. 2022, 2022, 9240569. [Google Scholar] [CrossRef] [PubMed]
- Sliwowska, J.H.; Fergani, C.; Gawałek, M.; Skowronska, B.; Fichna, P.; Lehman, M.N. Insulin: Its Role in the Central Control of Reproduction. Physiol. Behav. 2014, 133, 197–206. [Google Scholar] [CrossRef] [PubMed]
- Vatier, C.; Christin-Maitre, S.; Vigouroux, C. Role of Insulin Resistance on Fertility—Focus on Polycystic Ovary Syndrome. Ann. Endocrinol. 2022, 83, 199–202. [Google Scholar] [CrossRef]
- Patel, S. Polycystic Ovary Syndrome (PCOS), an Inflammatory, Systemic, Lifestyle Endocrinopathy. J. Steroid Biochem. Mol. Biol. 2018, 182, 27–36. [Google Scholar] [CrossRef]
- Foroozanfard, F.; Jamilian, M.; Jafari, Z.; Khassaf, A.; Hosseini, A.; Khorammian, H.; Asemi, Z. Effects of Zinc Supplementation on Markers of Insulin Resistance and Lipid Profiles in Women with Polycystic Ovary Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Exp. Clin. Endocrinol. Diabetes 2015, 123, 215–220. [Google Scholar] [PubMed]
- Mazaheri Nia, L.; Iravani, M.; Abedi, P.; Cheraghian, B. Effect of Zinc on Testosterone Levels and Sexual Function of Postmenopausal Women: A Randomized Controlled Trial. J. Sex Marital Ther. 2021, 47, 804–813. [Google Scholar] [CrossRef] [PubMed]
- Klug, A. Zinc Finger Peptides for the Regulation of Gene Expression. J. Mol. Biol. 1999, 293, 215–218. [Google Scholar] [CrossRef] [PubMed]
- Favier, A.E. The Role of Zinc in Reproduction. Hormonal Mechanisms. Biol. Trace Elem. Res. 1992, 32, 363–382. [Google Scholar] [CrossRef] [PubMed]
- Michos, C.; Kalfakakou, V.; Karkabounas, S.; Kiortsis, D.; Evangelou, A. Changes in Copper and Zinc Plasma Concentrations during the Normal Menstrual Cycle in Women. Gynecol. Endocrinol. 2010, 26, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Scholl, T.O.; Hediger, M.L.; Schall, J.I.; Fischer, R.L.; Khoo, C.S. Low Zinc Intake during Pregnancy: Its Association with Preterm and Very Preterm Delivery. Am. J. Epidemiol. 1993, 137, 1115–1124. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Hu, Y.-F.; Hao, J.-H.; Chen, Y.-H.; Su, P.-Y.; Wang, Y.; Yu, Z.; Fu, L.; Xu, Y.-Y.; Zhang, C.; et al. Maternal Zinc Deficiency during Pregnancy Elevates the Risks of Fetal Growth Restriction: A Population-Based Birth Cohort Study. Sci. Rep. 2015, 5, 11262. [Google Scholar] [CrossRef] [PubMed]
- Neggers, Y.H.; Cutter, G.R.; Acton, R.T.; Alvarez, J.O.; Bonner, J.L.; Goldenberg, R.L.; Go, R.C.; Roseman, J.M. A Positive Association between Maternal Serum Zinc Concentration and Birth Weight. Am. J. Clin. Nutr. 1990, 51, 678–684. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.R.; Wahlin-Jacobsen, S. Testosterone in Women--the Clinical Significance. Lancet Diabetes Endocrinol. 2015, 3, 980–992. [Google Scholar] [CrossRef]
- Rothman, M.S.; Carlson, N.E.; Xu, M.; Wang, C.; Swerdloff, R.; Lee, P.; Goh, V.H.H.; Ridgway, E.C.; Wierman, M.E. Reexamination of Testosterone, Dihydrotestosterone, Estradiol and Estrone Levels across the Menstrual Cycle and in Postmenopausal Women Measured by Liquid Chromatography–tandem Mass Spectrometry. Steroids 2011, 76, 177–182. [Google Scholar] [CrossRef]
- Xiao, L.; Yang, C.; Gu, W.; Liu, R.; Chen, D. Associations between Serum Copper, Zinc, Selenium Level and Sex Hormones among 6-19 Years Old Children and Adolescents in NHANES 2013–2016. Front. Endocrinol. 2022, 13, 924338. [Google Scholar] [CrossRef] [PubMed]
- Oh, Y.; Chung, K.C. Zinc Finger Protein 131 Inhibits Estrogen Signaling by Suppressing Estrogen Receptor α Homo-Dimerization. Biochem. Biophys. Res. Commun. 2013, 430, 400–405. [Google Scholar] [CrossRef] [PubMed]
- Arao, Y.; Korach, K.S. The Physiological Role of Estrogen Receptor Functional Domains. Essays Biochem. 2021, 65, 867–875. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Anthony, K.; Diaz, F.J. Transition Metal Chelator Induces Progesterone Production in Mouse Cumulus-Oocyte Complexes and Corpora Lutea. Biol. Trace Elem. Res. 2017, 176, 374–383. [Google Scholar] [CrossRef] [PubMed]
- Barile, G.; Sica, G.; Montemurro, A.; Iacobelli, S.; Corradini, M. Levels of Estrogen and Progesterone Receptor in Human Endometrium during the Menstrual Cycle. Eur. J. Obstet. Gynecol. Reprod. Biol. 1979, 9, 243–246. [Google Scholar] [CrossRef] [PubMed]
- Duncan, F.E.; Que, E.L.; Zhang, N.; Feinberg, E.C.; O’Halloran, T.V.; Woodruff, T.K. The Zinc Spark Is an Inorganic Signature of Human Egg Activation. Sci. Rep. 2016, 6, 24737. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Diaz, F.J. Acute Dietary Zinc Deficiency before Conception Compromises Oocyte Epigenetic Programming and Disrupts Embryonic Development. Dev. Biol. 2013, 376, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Lisle, R.S.; Anthony, K.; Randall, M.A.; Diaz, F.J. Oocyte-Cumulus Cell Interactions Regulate Free Intracellular Zinc in Mouse Oocytes. Reproduction 2013, 145, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Que, E.L.; Bleher, R.; Duncan, F.E.; Kong, B.Y.; Gleber, S.C.; Vogt, S.; Chen, S.; Garwin, S.A.; Bayer, A.R.; Dravid, V.P.; et al. Quantitative Mapping of Zinc Fluxes in the Mammalian Egg Reveals the Origin of Fertilization-Induced Zinc Sparks. Nat. Chem. 2015, 7, 130–139. [Google Scholar] [CrossRef]
- Kim, A.M.; Vogt, S.; O’Halloran, T.V.; Woodruff, T.K. Zinc Availability Regulates Exit from Meiosis in Maturing Mammalian Oocytes. Nat. Chem. Biol. 2010, 6, 674–681. [Google Scholar] [CrossRef]
- Que, E.L.; Duncan, F.E.; Bayer, A.R.; Philips, S.J.; Roth, E.W.; Bleher, R.; Gleber, S.C.; Vogt, S.; Woodruff, T.K.; O’Halloran, T.V. Zinc Sparks Induce Physiochemical Changes in the Egg Zona Pellucida That Prevent Polyspermy. Integr. Biol. 2017, 9, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Bernhardt, M.L.; Kong, B.Y.; Kim, A.M.; O’Halloran, T.V.; Woodruff, T.K. A Zinc-Dependent Mechanism Regulates Meiotic Progression in Mammalian Oocytes. Biol. Reprod. 2012, 86, 114. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Diaz, F.J. Zinc Depletion Causes Multiple Defects in Ovarian Function during the Periovulatory Period in Mice. Endocrinology 2012, 153, 873–886. [Google Scholar] [CrossRef] [PubMed]
- Kong, B.Y.; Bernhardt, M.L.; Kim, A.M.; O’Halloran, T.V.; Woodruff, T.K. Zinc Maintains Prophase I Arrest in Mouse Oocytes through Regulation of the MOS-MAPK Pathway. Biol. Reprod. 2012, 87, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Ebisch, I.M.W.; Thomas, C.M.G.; Peters, W.H.M.; Braat, D.D.M.; Steegers-Theunissen, R.P.M. The Importance of Folate, Zinc and Antioxidants in the Pathogenesis and Prevention of Subfertility. Hum. Reprod. Update 2007, 13, 163–174. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Wactawski-Wende, J.; Michels, K.A.; Schliep, K.C.; Plowden, T.C.; Chaljub, E.N.; Mumford, S.L. Dietary Minerals, Reproductive Hormone Levels and Sporadic Anovulation: Associations in Healthy Women with Regular Menstrual Cycles. Br. J. Nutr. 2018, 120, 81–89. [Google Scholar] [CrossRef]
- Akinloye, O.; Abbiyesuku, F.M.; Oguntibeju, O.O.; Arowojolu, A.O.; Truter, E.J. The Impact of Blood and Seminal Plasma Zinc and Copper Concentrations on Spermogram and Hormonal Changes in Infertile Nigerian Men. Reprod. Biol. 2011, 11, 83–98. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Karunanithy, R.; Edirisinghe, W.R.; Roy, A.C.; Wong, P.C.; Ratnam, S.S. Human Follicular Fluid Levels of Calcium, Copper and Zinc. Gynecol. Obstet. Investig. 1987, 23, 129–132. [Google Scholar] [CrossRef]
- Menezo, Y.; Khatchadourian, C.; Gharib, A.; Hamidi, J.; Greenland, T.; Sarda, N. Regulation of S-Adenosyl Methionine Synthesis in the Mouse Embryo. Life Sci. 1989, 44, 1601–1609. [Google Scholar] [CrossRef]
- Zheng, G.; Wang, L.; Guo, Z.; Sun, L.; Wang, L.; Wang, C.; Zuo, Z.; Qiu, H. Association of Serum Heavy Metals and Trace Element Concentrations with Reproductive Hormone Levels and Polycystic Ovary Syndrome in a Chinese Population. Biol. Trace Elem. Res. 2015, 167, 1–10. [Google Scholar] [CrossRef]
- Özkaya, M.O.; Nazıroğlu, M.; Barak, C.; Berkkanoglu, M. Effects of Multivitamin/mineral Supplementation on Trace Element Levels in Serum and Follicular Fluid of Women Undergoing in Vitro Fertilization (IVF). Biol. Trace Elem. Res. 2011, 139, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kanafchian, M.; Mahjoub, S.; Esmaeilzadeh, S.; Rahsepar, M.; Mosapour, A. Status of Serum Selenium and Zinc in Patients with the Polycystic Ovary Syndrome with and without Insulin Resistance. Middle East Fertil. Soc. J. 2018, 23, 241–245. [Google Scholar] [CrossRef]
- Özer, A.; Bakacak, M.; Kıran, H.; Ercan, Ö.; Köstü, B.; Kanat-Pektaş, M.; Kılınç, M.; Aslan, F. Increased Oxidative Stress Is Associated with Insulin Resistance and Infertility in Polycystic Ovary Syndrome. Ginekol. Pol. 2016, 87, 733–738. [Google Scholar] [CrossRef] [PubMed]
- Cruz, K.J.C.; de Oliveira, A.R.S.; Morais, J.B.S.; Severo, J.S.; Mendes, P.M.V.; de Sousa Melo, S.R.; de Sousa, G.S.; Marreiro, D. do N. Zinc and Insulin Resistance: Biochemical and Molecular Aspects. Biol. Trace Elem. Res. 2018, 186, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Olechnowicz, J.; Tinkov, A.; Skalny, A.; Suliburska, J. Zinc Status Is Associated with Inflammation, Oxidative Stress, Lipid, and Glucose Metabolism. J. Physiol. Sci. 2018, 68, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Tańska, K.; Gietka-Czernel, M.; Glinicki, P.; Kozakowski, J. Thyroid Autoimmunity and Its Negative Impact on Female Fertility and Maternal Pregnancy Outcomes. Front. Endocrinol. 2022, 13, 1049665. [Google Scholar] [CrossRef] [PubMed]
- Stuss, M.; Michalska-Kasiczak, M.; Sewerynek, E. The Role of Selenium in Thyroid Gland Pathophysiology. Endokrynol. Pol. 2017, 68, 440–465. [Google Scholar] [CrossRef] [PubMed]
- Köhrle, J. Selenium and the Thyroid. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Bucci, I.; Giuliani, C.; Di Dalmazi, G.; Formoso, G.; Napolitano, G. Thyroid Autoimmunity in Female Infertility and Assisted Reproductive Technology Outcome. Front. Endocrinol. 2022, 13, 768363. [Google Scholar] [CrossRef]
- Goldsmith, R.E.; Sturgis, S.H.; Lerman, J.; Stanbury, J.B. The Menstrual Pattern in Thyroid Disease. J. Clin. Endocrinol. Metab. 1952, 12, 846–855. [Google Scholar] [CrossRef]
- Koutras, D.A. Disturbances of Menstruation in Thyroid Disease. Ann. N. Y. Acad. Sci. 1997, 816, 280–284. [Google Scholar] [CrossRef] [PubMed]
- Fedail, J.S.; Zheng, K.; Wei, Q.; Kong, L.; Shi, F. Roles of Thyroid Hormones in Follicular Development in the Ovary of Neonatal and Immature Rats. Endocrine 2014, 46, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Poppe, K.; Glinoer, D. Thyroid Autoimmunity and Hypothyroidism before and during Pregnancy. Hum. Reprod. Update 2003, 9, 149–161. [Google Scholar] [CrossRef] [PubMed]
- Silva, J.F.; Ocarino, N.M.; Serakides, R. Thyroid Hormones and Female Reproduction. Biol. Reprod. 2018, 99, 907–921. [Google Scholar] [CrossRef] [PubMed]
- Mintziori, G.; Kita, M.; Duntas, L.; Goulis, D.G. Consequences of Hyperthyroidism in Male and Female Fertility: Pathophysiology and Current Management. J. Endocrinol. Investig. 2016, 39, 849–853. [Google Scholar] [CrossRef] [PubMed]
- Vissenberg, R.; Manders, V.D.; Mastenbroek, S.; Fliers, E.; Afink, G.B.; Ris-Stalpers, C.; Goddijn, M.; Bisschop, P.H. Pathophysiological Aspects of Thyroid Hormone Disorders/thyroid Peroxidase Autoantibodies and Reproduction. Hum. Reprod. Update 2015, 21, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Dittrich, R.; Beckmann, M.W.; Oppelt, P.G.; Hoffmann, I.; Lotz, L.; Kuwert, T.; Mueller, A. Thyroid Hormone Receptors and Reproduction. J. Reprod. Immunol. 2011, 90, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Zagrodzki, P.; Ratajczak, R.; Wietecha-Posłuszny, R. The Interaction between Selenium Status, Sex Hormones, and Thyroid Metabolism in Adolescent Girls in the Luteal Phase of Their Menstrual Cycle. Biol. Trace Elem. Res. 2007, 120, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Zagrodzki, P.; Ratajczak, R. Selenium Status, Sex Hormones, and Thyroid Function in Young Women. J. Trace Elem. Med. Biol. 2008, 22, 296–304. [Google Scholar] [CrossRef]
- Guastamacchia, E.; Giagulli, V.A.; Licchelli, B.; Triggiani, V. Selenium and Iodine in Autoimmune Thyroiditis. Endocr. Metab. Immune Disord. Drug Targets 2015, 15, 288–292. [Google Scholar] [CrossRef]
- Krassas, G.E.; Pontikides, N.; Kaltsas, T.; Papadopoulou, P.; Paunkovic, J.; Paunkovic, N.; Duntas, L.H. Disturbances of Menstruation in Hypothyroidism. Clin. Endocrinol. 1999, 50, 655–659. [Google Scholar] [CrossRef] [PubMed]
- Mills, J.L.; Buck Louis, G.M.; Kannan, K.; Weck, J.; Wan, Y.; Maisog, J.; Giannakou, A.; Wu, Q.; Sundaram, R. Delayed Conception in Women with Low-Urinary Iodine Concentrations: A Population-Based Prospective Cohort Study. Hum. Reprod. 2018, 33, 426–433. [Google Scholar] [CrossRef] [PubMed]
- Mathews, D.M.; Johnson, N.P.; Sim, R.G.; O’Sullivan, S.; Peart, J.M.; Hofman, P.L. Iodine and Fertility: Do We Know Enough? Hum. Reprod. 2021, 36, 265–274. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.N.; Albrecht, D.; Scholz, A.; Gutierrez-Buey, G.; Lazarus, J.H.; Dayan, C.M.; Okosieme, O.E. Global Epidemiology of Hyperthyroidism and Hypothyroidism. Nat. Rev. Endocrinol. 2018, 14, 301–316. [Google Scholar] [CrossRef] [PubMed]
- Dunn, J.T.; Delange, F. Damaged Reproduction: The Most Important Consequence of Iodine Deficiency. J. Clin. Endocrinol. Metab. 2001, 86, 2360–2363. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Diaz, E.; Pearce, E.N. Iodine Status and Supplementation Before, during, and after Pregnancy. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101430. [Google Scholar] [CrossRef]
- Sorrenti, S.; Baldini, E.; Pironi, D.; Lauro, A.; D’Orazi, V.; Tartaglia, F.; Tripodi, D.; Lori, E.; Gagliardi, F.; Praticò, M.; et al. Iodine: Its Role in Thyroid Hormone Biosynthesis and Beyond. Nutrients 2021, 13, 4469. [Google Scholar] [CrossRef] [PubMed]
- Joshi, J.V.; Bhandarkar, S.D.; Chadha, M.; Balaiah, D.; Shah, R. Menstrual Irregularities and Lactation Failure May Precede Thyroid Dysfunction or Goitre. J. Postgrad. Med. 1993, 39, 137–141. [Google Scholar]
- Rosner, W.; Hryb, D.J.; Khan, M.S.; Nakhla, A.M.; Romas, N.A. Sex Hormone-Binding Globulin: Anatomy and Physiology of a New Regulatory System. J. Steroid Biochem. Mol. Biol. 1991, 40, 813–820. [Google Scholar] [CrossRef]
- Zhu, J.-L.; Chen, Z.; Feng, W.-J.; Long, S.-L.; Mo, Z.-C. Sex Hormone-Binding Globulin and Polycystic Ovary Syndrome. Clin. Chim. Acta 2019, 499, 142–148. [Google Scholar] [CrossRef]
- Unuane, D.; Velkeniers, B. Impact of Thyroid Disease on Fertility and Assisted Conception. Best Pract. Res. Clin. Endocrinol. Metab. 2020, 34, 101378. [Google Scholar] [CrossRef] [PubMed]
- Duffy, D.M.; Ko, C.; Jo, M.; Brannstrom, M.; Curry, T.E. Ovulation: Parallels with Inflammatory Processes. Endocr. Rev. 2019, 40, 369–416. [Google Scholar] [CrossRef] [PubMed]
- Holesh, J.E.; Bass, A.N.; Lord, M. Physiology, Ovulation. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Kanasaki, H.; Oride, A.; Mijiddorj, T.; Kyo, S. Role of Thyrotropin-Releasing Hormone in Prolactin-Producing Cell Models. Neuropeptides 2015, 54, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Castillo, J.C.; Haahr, T.; Martínez-Moya, M.; Humaidan, P. Gonadotropin-Releasing Hormone Agonist for Ovulation Trigger—OHSS Prevention and Use of Modified Luteal Phase Support for Fresh Embryo Transfer. Upsala J. Med. Sci. 2020, 125, 131–137. [Google Scholar] [CrossRef] [PubMed]
- Karsch, F.J.; Bowen, J.M.; Caraty, A.; Evans, N.P.; Moenter, S.M. Gonadotropin-Releasing Hormone Requirements for Ovulation. Biol. Reprod. 1997, 56, 303–309. [Google Scholar] [CrossRef]
- Matsuzaki, T.; Azuma, K.; Irahara, M.; Yasui, T.; Aono, T. Mechanism of Anovulation in Hyperprolactinemic Amenorrhea Determined by Pulsatile Gonadotropin-Releasing Hormone Injection Combined with Human Chorionic Gonadotropin. Fertil. Steril. 1994, 62, 1143–1149. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, U.B. Hyperprolactinemia and Infertility: New Insights. J. Clin. Investig. 2012, 122, 3467–3468. [Google Scholar] [CrossRef]
- Vogt, A.-C.S.; Arsiwala, T.; Mohsen, M.; Vogel, M.; Manolova, V.; Bachmann, M.F. On Iron Metabolism and Its Regulation. Int. J. Mol. Sci. 2021, 22, 4591. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Xu, M.-M.; Wang, J.; Xie, J.-X. Effect of Estrogen on Iron Metabolism in Mammals. Sheng Li Xue Bao 2016, 68, 637–643. [Google Scholar]
- Hamad, M.; Bajbouj, K.; Taneera, J. The Case for an Estrogen-Iron Axis in Health and Disease. Exp. Clin. Endocrinol. Diabetes 2020, 128, 270–277. [Google Scholar] [CrossRef]
- Song, Y.-S.; Annalora, A.J.; Marcus, C.B.; Jefcoate, C.R.; Sorenson, C.M.; Sheibani, N. Cytochrome P450 1B1: A Key Regulator of Ocular Iron Homeostasis and Oxidative Stress. Cells 2022, 11, 2930. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, C.; Tsuchiya, K.; Maeda, K. Hypoxia-Inducible Factor Prolyl Hydroxylase Inhibitors and Iron Metabolism. Int. J. Mol. Sci. 2023, 24, 3037. [Google Scholar] [CrossRef] [PubMed]
- Vranka, J.A.; Sakai, L.Y.; Bächinger, H.P. Prolyl 3-Hydroxylase 1, Enzyme Characterization and Identification of a Novel Family of Enzymes. J. Biol. Chem. 2004, 279, 23615–23621. [Google Scholar] [CrossRef] [PubMed]
- Pihlajaniemi, T.; Myllylä, R.; Kivirikko, K.I. Prolyl 4-Hydroxylase and Its Role in Collagen Synthesis. J. Hepatol. 1991, 13 (Suppl. S3), S2–S7. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.-W.; Lai, Z.-Z.; Yang, H.-L.; Yang, S.-L.; Wang, C.-J.; Ao, D.; Ruan, L.-Y.; Shen, H.-H.; Zhou, W.-J.; Mei, J.; et al. Collagen at the Maternal-Fetal Interface in Human Pregnancy. Int. J. Biol. Sci. 2020, 16, 2220–2234. [Google Scholar] [CrossRef] [PubMed]
- Bronner, F. Extracellular and Intracellular Regulation of Calcium Homeostasis. Sci. World J. 2001, 1, 919–925. [Google Scholar] [CrossRef] [PubMed]
- Vannucci, L.; Fossi, C.; Quattrini, S.; Guasti, L.; Pampaloni, B.; Gronchi, G.; Giusti, F.; Romagnoli, C.; Cianferotti, L.; Marcucci, G.; et al. Calcium Intake in Bone Health: A Focus on Calcium-Rich Mineral Waters. Nutrients 2018, 10, 1930. [Google Scholar] [CrossRef] [PubMed]
- Petersen, O.H.; Petersen, C.C.; Kasai, H. Calcium and Hormone Action. Annu. Rev. Physiol. 1994, 56, 297–319. [Google Scholar] [CrossRef] [PubMed]
- Südhof, T.C. Calcium Control of Neurotransmitter Release. Cold Spring Harb. Perspect. Biol. 2012, 4, a011353. [Google Scholar] [CrossRef]
- Jasoni, C.L.; Romanò, N.; Constantin, S.; Lee, K.; Herbison, A.E. Calcium Dynamics in Gonadotropin-Releasing Hormone Neurons. Front. Neuroendocrinol. 2010, 31, 259–269. [Google Scholar] [CrossRef]
- Pitkin, R.M.; Reynolds, W.A.; Williams, G.A.; Hargis, G.K. Calcium-Regulating Hormones during the Menstrual Cycle. J. Clin. Endocrinol. Metab. 1978, 47, 626–632. [Google Scholar] [CrossRef]
- Kadoura, S.; Alhalabi, M.; Nattouf, A.H. Effect of Calcium and Vitamin D Supplements as an Adjuvant Therapy to Metformin on Menstrual Cycle Abnormalities, Hormonal Profile, and IGF-1 System in Polycystic Ovary Syndrome Patients: A Randomized, Placebo-Controlled Clinical Trial. Adv. Pharmacol. Sci. 2019, 2019, 9680390. [Google Scholar] [CrossRef]
- Williams, C.L.; Smith, S.M. Calcium Dependence of Spontaneous Neurotransmitter Release. J. Neurosci. Res. 2018, 96, 335–347. [Google Scholar] [CrossRef] [PubMed]
- Bazybek, N.; Wei, Y.; Ma, G. Advances in Encapsulating Gonadotropin-Releasing Hormone Agonists for Controlled Release: A Review. J. Microencapsul. 2022, 39, 452–466. [Google Scholar] [CrossRef]
- Scheuer, R.; Philipp, S.E.; Becker, A.; Nalbach, L.; Ampofo, E.; Montenarh, M.; Götz, C. Protein Kinase CK2 Controls Ca2.1-Dependent Calcium Currents and Insulin Release in Pancreatic β-Cells. Int. J. Mol. Sci. 2020, 21, 4668. [Google Scholar] [CrossRef] [PubMed]
- Tokarz, V.L.; MacDonald, P.E.; Klip, A. The Cell Biology of Systemic Insulin Function. J. Cell Biol. 2018, 217, 2273–2289. [Google Scholar] [CrossRef]
- Bettocchi, C.; Rinaldi, M.; Sebastiani, F. GnRH in the Treatment of Hypogonadotropic Hypogonadism. Curr. Pharm. Des. 2021, 27, 2754–2756. [Google Scholar] [CrossRef]
- Barabás, K.; Szabó-Meleg, E.; Ábrahám, I.M. Effect of Inflammation on Female Gonadotropin-Releasing Hormone (GnRH) Neurons: Mechanisms and Consequences. Int. J. Mol. Sci. 2020, 21, 529. [Google Scholar] [CrossRef] [PubMed]
- Gröber, U.; Schmidt, J.; Kisters, K. Magnesium in Prevention and Therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef]
- Hayashi, T.; Harada, N. Post-Translational Dual Regulation of Cytochrome P450 Aromatase at the Catalytic and Protein Levels by Phosphorylation/dephosphorylation. FEBS J. 2014, 281, 4830–4840. [Google Scholar] [CrossRef]
- Balthazart, J.; Baillien, M.; Charlier, T.D.; Cornil, C.A.; Ball, G.F. Multiple Mechanisms Control Brain Aromatase Activity at the Genomic and Non-Genomic Level. J. Steroid Biochem. Mol. Biol. 2003, 86, 367–379. [Google Scholar] [CrossRef]
- Nelson, L.R.; Bulun, S.E. Estrogen Production and Action. J. Am. Acad. Dermatol. 2001, 45, S116–S124. [Google Scholar] [CrossRef] [PubMed]
- Kauffman, R.P.; Tullar, P.E.; Nipp, R.D.; Castracane, V.D. Serum Magnesium Concentrations and Metabolic Variables in Polycystic Ovary Syndrome. Acta Obstet. Gynecol. Scand. 2011, 90, 452–458. [Google Scholar] [CrossRef]
- Chakraborty, P.; Ghosh, S.; Goswami, S.K.; Kabir, S.N.; Chakravarty, B.; Jana, K. Altered Trace Mineral Milieu Might Play an Aetiological Role in the Pathogenesis of Polycystic Ovary Syndrome. Biol. Trace Elem. Res. 2013, 152, 9–15. [Google Scholar] [CrossRef]
- Kanafchian, M.; Esmaeilzadeh, S.; Mahjoub, S.; Rahsepar, M.; Ghasemi, M. Status of Serum Copper, Magnesium, and Total Antioxidant Capacity in Patients with Polycystic Ovary Syndrome. Biol. Trace Elem. Res. 2020, 193, 111–117. [Google Scholar] [CrossRef]
- Sharma, P.; Kapoor, H.S.; Kaur, B.; Kamra, P.; Khetarpal, P. Investigation of the Association of Serum Trace Elements Concentrations and Serum Biochemical Parameters with the Risk of Polycystic Ovary Syndrome: A Case-Control Study. Biol. Trace Elem. Res. 2023, 202, 73–86. [Google Scholar] [CrossRef]
- Hruby, A.; Meigs, J.B.; O’Donnell, C.J.; Jacques, P.F.; McKeown, N.M. Higher Magnesium Intake Reduces Risk of Impaired Glucose and Insulin Metabolism and Progression from Prediabetes to Diabetes in Middle-Aged Americans. Diabetes Care 2014, 37, 419–427. [Google Scholar] [CrossRef]
- Gommers, L.M.M.; Hoenderop, J.G.J.; Bindels, R.J.M.; de Baaij, J.H.F. Hypomagnesemia in Type 2 Diabetes: A Vicious Circle? Diabetes 2016, 65, 3–13. [Google Scholar] [CrossRef]
- Kostov, K. Effects of Magnesium Deficiency on Mechanisms of Insulin Resistance in Type 2 Diabetes: Focusing on the Processes of Insulin Secretion and Signaling. Int. J. Mol. Sci. 2019, 20, 1351. [Google Scholar] [CrossRef] [PubMed]
- Noori, N.; Nafar, M.; Poorrezagholi, F.; Ahmadpoor, P.; Samadian, F.; Firouzan, A.; Einollahi, B. Dietary Intakes of Fiber and Magnesium and Incidence of Metabolic Syndrome in First Year after Renal Transplantation. J. Ren. Nutr. 2010, 20, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, D.P.; Sharma, R.; Bansal, D.D. Implications of Magnesium Deficiency in Type 2 Diabetes: A Review. Biol. Trace Elem. Res. 2010, 134, 119–129. [Google Scholar] [CrossRef]
- Simental-Mendía, L.E.; Sahebkar, A.; Rodríguez-Morán, M.; Guerrero-Romero, F. A Systematic Review and Meta-Analysis of Randomized Controlled Trials on the Effects of Magnesium Supplementation on Insulin Sensitivity and Glucose Control. Pharmacol. Res. 2016, 111, 272–282. [Google Scholar] [CrossRef]
- Meier, R.K. Polycystic Ovary Syndrome. Nurs. Clin. N. Am. 2018, 53, 407–420. [Google Scholar] [CrossRef]
- Hamilton, K.P.; Zelig, R.; Parker, A.R.; Haggag, A. Insulin Resistance and Serum Magnesium Concentrations among Women with Polycystic Ovary Syndrome. Curr. Dev. Nutr. 2019, 3, nzz108. [Google Scholar] [CrossRef]
- Jamilian, M.; Maktabi, M.; Asemi, Z. A Trial on The Effects of Magnesium-Zinc-Calcium-Vitamin D Co-Supplementation on Glycemic Control and Markers of Cardio-Metabolic Risk in Women with Polycystic Ovary Syndrome. Arch. Iran. Med. 2017, 20, 640–645. [Google Scholar]
- Szczuko, M.; Skowronek, M.; Zapałowska-Chwyć, M.; Starczewski, A. Quantitative Assessment of Nutrition in Patients with Polycystic Ovary Syndrome (PCOS). Rocz. Panstw. Zakl. Hig. 2016, 67, 419–426. [Google Scholar]
- Luo, X.; Cai, W.-Y.; Ma, H.-L.; Cong, J.; Chang, H.; Gao, J.-S.; Shen, W.-J.; Wang, Y.; Yang, X.-M.; Wu, X.-K. Associations of Serum Magnesium With Insulin Resistance and Testosterone in Women With Polycystic Ovary Syndrome. Front. Endocrinol. 2021, 12, 683040. [Google Scholar] [CrossRef]
- Shahmoradi, S.; Chiti, H.; Tavakolizadeh, M.; Hatami, R.; Motamed, N.; Ghaemi, M. The Effect of Magnesium Supplementation on Insulin Resistance and Metabolic Profiles in Women with Polycystic Ovary Syndrome: A Randomized Clinical Trial. Biol. Trace Elem. Res. 2023, 202, 941–946. [Google Scholar] [CrossRef]
- Leong, I. Reproductive Endocrinology: Restoring Ovarian Function. Nat. Rev. Endocrinol. 2018, 14, 66. [Google Scholar] [CrossRef] [PubMed]
- Baerwald, A.R.; Adams, G.P.; Pierson, R.A. Ovarian Antral Folliculogenesis during the Human Menstrual Cycle: A Review. Hum. Reprod. Update 2012, 18, 73–91. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Gupta, S.; Sharma, R.K. Role of Oxidative Stress in Female Reproduction. Reprod. Biol. Endocrinol. 2005, 3, 28. [Google Scholar] [CrossRef]
- Homer, H.A. The Role of Oocyte Quality in Explaining “Unexplained” Infertility. Semin. Reprod. Med. 2020, 38, 21–28. [Google Scholar] [CrossRef]
- Chou, C.-H.; Chen, M.-J. The Effect of Steroid Hormones on Ovarian Follicle Development. Vitam. Horm. 2018, 107, 155–175. [Google Scholar]
- Piette, P. The History of Natural Progesterone, the Never-Ending Story. Climacteric 2018, 21, 308–314. [Google Scholar] [CrossRef]
- Kagawa, H.; Sakurai, Y.; Horiuchi, R.; Kazeto, Y.; Gen, K.; Imaizumi, H.; Masuda, Y. Mechanism of Oocyte Maturation and Ovulation and Its Application to Seed Production in the Japanese Eel. Fish Physiol. Biochem. 2013, 39, 13–17. [Google Scholar] [CrossRef]
- Maggi, R.; Cariboni, A.M.; Marelli, M.M.; Moretti, R.M.; Andrè, V.; Marzagalli, M.; Limonta, P. GnRH and GnRH Receptors in the Pathophysiology of the Human Female Reproductive System. Hum. Reprod. Update 2016, 22, 358–381. [Google Scholar] [CrossRef]
- Sánchez, F.; Smitz, J. Molecular Control of Oogenesis. Biochim. Biophys. Acta 2012, 1822, 1896–1912. [Google Scholar] [CrossRef]
- Krajnik, K.; Mietkiewska, K.; Skowronska, A.; Kordowitzki, P.; Skowronski, M.T. Oogenesis in Women: From Molecular Regulatory Pathways and Maternal Age to Stem Cells. Int. J. Mol. Sci. 2023, 24, 6837. [Google Scholar] [CrossRef]
- Tosti, E. Calcium Ion Currents Mediating Oocyte Maturation Events. Reprod. Biol. Endocrinol. 2006, 4, 26. [Google Scholar] [CrossRef]
- Homa, S.T.; Carroll, J.; Swann, K. The Role of Calcium in Mammalian Oocyte Maturation and Egg Activation. Hum. Reprod. 1993, 8, 1274–1281. [Google Scholar] [CrossRef]
- Boni, R.; Gualtieri, R.; Talevi, R.; Tosti, E. Calcium and Other Ion Dynamics during Gamete Maturation and Fertilization. Theriogenology 2007, 68 (Suppl. S1), S156–S164. [Google Scholar] [CrossRef]
- Silvestre, F.; Boni, R.; Fissore, R.A.; Tosti, E. Ca2+ Signaling during Maturation of Cumulus-Oocyte Complex in Mammals. Mol. Reprod. Dev. 2011, 78, 744–756. [Google Scholar] [CrossRef]
- Machaca, K. Ca2+ Signaling Differentiation during Oocyte Maturation. J. Cell. Physiol. 2007, 213, 331–340. [Google Scholar] [CrossRef]
- Ducibella, T.; Huneau, D.; Angelichio, E.; Xu, Z.; Schultz, R.M.; Kopf, G.S.; Fissore, R.; Madoux, S.; Ozil, J.-P. Egg-to-Embryo Transition Is Driven by Differential Responses to Ca2+ Oscillation Number. Dev. Biol. 2002, 250, 280–291. [Google Scholar] [CrossRef]
- Martín-Romero, F.J.; López-Guerrero, A.M.; Alvarez, I.S.; Pozo-Guisado, E. Role of Store-Operated Calcium Entry during Meiotic Progression and Fertilization of Mammalian Oocytes. Int. Rev. Cell Mol. Biol. 2012, 295, 291–328. [Google Scholar]
- Madgwick, S.; Levasseur, M.; Jones, K.T. Calmodulin-Dependent Protein Kinase II, and Not Protein Kinase C, Is Sufficient for Triggering Cell-Cycle Resumption in Mammalian Eggs. J. Cell Sci. 2005, 118, 3849–3859. [Google Scholar] [CrossRef]
- Lefèvre, B.; Pesty, A.; Courtot, A.-M.; Martins, C.V.C.; Broca, O.; Denys, A.; Arnault, E.; Poirot, C.; Avazeri, N. The Phosphoinositide-Phospholipase C (PI-PLC) Pathway in the Mouse Oocyte. Crit. Rev. Eukaryot. Gene Expr. 2007, 17, 259–269. [Google Scholar] [CrossRef]
- Webb, S.E.; Miller, A.L. Calcium Signalling during Zebrafish Embryonic Development. Bioessays 2000, 22, 113–123. [Google Scholar] [CrossRef]
- Islam, M.S. Calcium Signaling: From Basic to Bedside. Adv. Exp. Med. Biol. 2020, 1131, 1–6. [Google Scholar]
- Cao, X.; Chen, Y. Mitochondria and Calcium Signaling in Embryonic Development. Semin. Cell Dev. Biol. 2009, 20, 337–345. [Google Scholar] [CrossRef]
- Chen, X.; Zhao, H.; Lv, J.; Dong, Y.; Zhao, M.; Sui, X.; Cui, R.; Liu, B.; Wu, K. Calcium Ionophore Improves Embryonic Development and Pregnancy Outcomes in Patients with Previous Developmental Problems in ICSI Cycles. BMC Pregnancy Childbirth 2022, 22, 894. [Google Scholar] [CrossRef] [PubMed]
- Takaya, J. Calcium-Deficiency during Pregnancy Affects Insulin Resistance in Offspring. Int. J. Mol. Sci. 2021, 22, 7008. [Google Scholar] [CrossRef] [PubMed]
- Korhonen, P.; Tihtonen, K.; Isojärvi, J.; Ojala, R.; Ashorn, U.; Ashorn, P.; Tammela, O. Calcium Supplementation during Pregnancy and Long-Term Offspring Outcome: A Systematic Literature Review and Meta-Analysis. Ann. N. Y. Acad. Sci. 2022, 1510, 36–51. [Google Scholar] [CrossRef] [PubMed]
- Appelman-Dijkstra, N.M.; Ertl, D.-A.; Zillikens, M.C.; Rjenmark, L.; Winter, E.M. Hypercalcemia during Pregnancy: Management and Outcomes for Mother and Child. Endocrine 2021, 71, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Ajong, A.B.; Kenfack, B.; Ali, I.M.; Yakum, M.N.; Ukaogo, P.O.; Mangala, F.N.; Aljerf, L.; Telefo, P.B. Calcium Supplementation in Pregnancy: An Analysis of Potential Determinants in an under-Resourced Setting. PLoS ONE 2023, 18, e0292303. [Google Scholar] [CrossRef] [PubMed]
- Yao, Y.; Tang, Y.; Qin, H.; Meng, R.; Zhang, C.; Zhang, Y.; Yang, Y.; Qiao, P.; Liu, J.; Su, J. Zinc Supplementation Promotes Oocyte Maturation and Subsequent Embryonic Development in Sheep. Theriogenology 2023, 206, 161–169. [Google Scholar] [CrossRef]
- Garner, T.B.; Hester, J.M.; Carothers, A.; Diaz, F.J. Role of Zinc in Female Reproduction. Biol. Reprod. 2021, 104, 976–994. [Google Scholar] [CrossRef] [PubMed]
- Petrucco, S.; Percudani, R. Structural Recognition of DNA by poly(ADP-Ribose)polymerase-like Zinc Finger Families. FEBS J. 2008, 275, 883–893. [Google Scholar] [CrossRef]
- Popović-Bijelić, A.; Kowol, C.R.; Lind, M.E.S.; Luo, J.; Himo, F.; Enyedy, E.A.; Arion, V.B.; Gräslund, A. Ribonucleotide Reductase Inhibition by Metal Complexes of Triapine (3-Aminopyridine-2-Carboxaldehyde Thiosemicarbazone): A Combined Experimental and Theoretical Study. J. Inorg. Biochem. 2011, 105, 1422–1431. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Kudo, H.; Suzuki, S.; Nemoto, N.; Sassa, S.; Sakamoto, S. Down Regulation by a Low-Zinc Diet in Gene Expression of Rat Prostatic Thymidylate Synthase and Thymidine Kinase. Nutr. Metab. 2008, 5, 12. [Google Scholar] [CrossRef]
- Wu, F.Y.; Wu, C.W. Zinc in DNA Replication and Transcription. Annu. Rev. Nutr. 1987, 7, 251–272. [Google Scholar] [CrossRef]
- MacDonald, R.S. The Role of Zinc in Growth and Cell Proliferation. J. Nutr. 2000, 130, 1500S–1508S. [Google Scholar] [CrossRef]
- Laity, J.H.; Lee, B.M.; Wright, P.E. Zinc Finger Proteins: New Insights into Structural and Functional Diversity. Curr. Opin. Struct. Biol. 2001, 11, 39–46. [Google Scholar] [CrossRef]
- Ha, J.-H.; Prela, O.; Carpizo, D.R.; Loh, S.N. p53 and Zinc: A Malleable Relationship. Front. Mol. Biosci. 2022, 9, 895887. [Google Scholar] [CrossRef]
- Beyersmann, D.; Haase, H. Functions of Zinc in Signaling, Proliferation and Differentiation of Mammalian Cells. Biometals 2001, 14, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Hester, J.; Hanna-Rose, W.; Diaz, F. Zinc Deficiency Reduces Fertility in C. Elegans Hermaphrodites and Disrupts Oogenesis and Meiotic Progression. Comp. Biochem. Physiol. C Toxicol. Pharmacol. 2017, 191, 203–209. [Google Scholar] [CrossRef]
- Liao, X.; Wu, L.; Yin, D.; Tian, D.; Zhou, C.; Liu, J.; Li, S.; Zhou, J.; Nie, Y.; Liao, H.; et al. The Role of Zinc in Follicular Development. Mol. Biol. Rep. 2023, 50, 4527–4534. [Google Scholar] [CrossRef]
- Jeon, Y.; Yoon, J.D.; Cai, L.; Hwang, S.-U.; Kim, E.; Zheng, Z.; Lee, E.; Kim, D.Y.; Hyun, S.-H. Supplementation of Zinc on Oocyte in Vitro Maturation Improves Preimplatation Embryonic Development in Pigs. Theriogenology 2014, 82, 866–874. [Google Scholar] [CrossRef] [PubMed]
- Kong, B.Y.; Duncan, F.E.; Que, E.L.; Xu, Y.; Vogt, S.; O’Halloran, T.V.; Woodruff, T.K. The Inorganic Anatomy of the Mammalian Preimplantation Embryo and the Requirement of Zinc during the First Mitotic Divisions. Dev. Dyn. 2015, 244, 935–947. [Google Scholar] [CrossRef] [PubMed]
- Hanna, L.A.; Clegg, M.S.; Momma, T.Y.; Daston, G.P.; Rogers, J.M.; Keen, C.L. Zinc Influences the in Vitro Development of Peri-Implantation Mouse Embryos. Birth Defects Res. A Clin. Mol. Teratol. 2003, 67, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Tian, X.; Diaz, F.J. Zinc Deficiency During Oocyte Maturation Causes Defects in Preimplantation Embryonic Development. Biol. Reprod. 2012, 87, 199. [Google Scholar] [CrossRef]
- Taylor, K.M.; Muraina, I.A.; Brethour, D.; Schmitt-Ulms, G.; Nimmanon, T.; Ziliotto, S.; Kille, P.; Hogstrand, C. Zinc Transporter ZIP10 Forms a Heteromer with ZIP6 Which Regulates Embryonic Development and Cell Migration. Biochem. J. 2016, 473, 2531–2544. [Google Scholar] [CrossRef]
- Kim, A.M.; Bernhardt, M.L.; Kong, B.Y.; Ahn, R.W.; Vogt, S.; Woodruff, T.K.; O’Halloran, T.V. Zinc Sparks Are Triggered by Fertilization and Facilitate Cell Cycle Resumption in Mammalian Eggs. ACS Chem. Biol. 2011, 6, 716–723. [Google Scholar] [CrossRef]
- Zhang, N.; Duncan, F.E.; Que, E.L.; O’Halloran, T.V.; Woodruff, T.K. The Fertilization-Induced Zinc Spark Is a Novel Biomarker of Mouse Embryo Quality and Early Development. Sci. Rep. 2016, 6, 22772. [Google Scholar] [CrossRef]
- Wooldridge, L.K.; Nardi, M.E.; Ealy, A.D. Zinc Supplementation during in Vitro Embryo Culture Increases Inner Cell Mass and Total Cell Numbers in Bovine blastocysts1. J. Anim. Sci. 2019, 97, 4946–4950. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.; Yoon, J.D.; Cai, L.; Hwang, S.-U.; Kim, E.; Zheng, Z.; Jeung, E.; Lee, E.; Hyun, S.-H. Zinc Deficiency during in Vitro Maturation of Porcine Oocytes Causes Meiotic Block and Developmental Failure. Mol. Med. Rep. 2015, 12, 5973–5982. [Google Scholar] [CrossRef] [PubMed]
- Janati, S.; Behmanesh, M.A.; Najafzadehvarzi, H.; Akhundzade, Z.; Poormoosavi, S.M. Follicular Fluid Zinc Level and Oocyte Maturity and Embryo Quality in Women with Polycystic Ovary Syndrome. Int. J. Fertil. Steril. 2021, 15, 197–201. [Google Scholar]
- Pang, W.; Leng, X.; Lu, H.; Yang, H.; Song, N.; Tan, L.; Jiang, Y.; Guo, C. Depletion of Intracellular Zinc Induces Apoptosis of Cultured Hippocampal Neurons through Suppression of ERK Signaling Pathway and Activation of Caspase-3. Neurosci. Lett. 2013, 552, 140–145. [Google Scholar] [CrossRef]
- Johnson-Wimbley, T.D.; Graham, D.Y. Diagnosis and Management of Iron Deficiency Anemia in the 21st Century. Therap. Adv. Gastroenterol. 2011, 4, 177–184. [Google Scholar] [CrossRef]
- Clark, A.R.; Stokes, Y.M. Follicle Structure Influences the Availability of Oxygen to the Oocyte in Antral Follicles. Comput. Math. Methods Med. 2011, 2011, 287186. [Google Scholar] [CrossRef]
- Liang, J.; Gao, Y.; Feng, Z.; Zhang, B.; Na, Z.; Li, D. Reactive Oxygen Species and Ovarian Diseases: Antioxidant Strategies. Redox Biol. 2023, 62, 102659. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, T.; Kyoya, T.; Nakamura, Y.; Sato, E.; Tomiyama, T.; Kyono, K. Oxygen Consumption Rate of Early Pre-Antral Follicles from Vitrified Human Ovarian Cortical Tissue. J. Reprod. Dev. 2014, 60, 460–467. [Google Scholar] [CrossRef] [PubMed]
- Georgieff, M.K. Iron Deficiency in Pregnancy. Am. J. Obstet. Gynecol. 2020, 223, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Georgieff, M.K.; Krebs, N.F.; Cusick, S.E. The Benefits and Risks of Iron Supplementation in Pregnancy and Childhood. Annu. Rev. Nutr. 2019, 39, 121–146. [Google Scholar] [CrossRef] [PubMed]
- Puig, S.; Ramos-Alonso, L.; Romero, A.M.; Martínez-Pastor, M.T. The Elemental Role of Iron in DNA Synthesis and Repair. Metallomics 2017, 9, 1483–1500. [Google Scholar] [CrossRef] [PubMed]
- Cheng, R.; Dhorajia, V.V.; Kim, J.; Kim, Y. Mitochondrial Iron Metabolism and Neurodegenerative Diseases. Neurotoxicology 2022, 88, 88–101. [Google Scholar] [CrossRef] [PubMed]
- Holzer, I.; Ott, J.; Beitl, K.; Mayrhofer, D.; Heinzl, F.; Ebenbauer, J.; Parry, J.P. Iron Status in Women with Infertility and Controls: A Case-Control Study. Front. Endocrinol. 2023, 14, 1173100. [Google Scholar] [CrossRef]
- Gonzalez-Martin, R.; Palomar, A.; Quiñonero, A.; Pellicer, N.; Fernandez-Saavedra, R.; Conde-Vilda, E.; Quejido, A.J.; Whitehead, C.; Scott, R.T., Jr.; Dominguez, F. The Impact of Essential Trace Elements on Ovarian Response and Reproductive Outcomes Following Single Euploid Embryo Transfer. Int. J. Mol. Sci. 2023, 24, 10968. [Google Scholar] [CrossRef] [PubMed]
- Liu, M.N.; Chen, L.; Xu, T.M.; Zhang, K. Potential Clinical Implications of Iron Metabolism in Ovarian Endometriosis. J. Trace Elem. Med. Biol. 2022, 73, 127017. [Google Scholar] [CrossRef]
- Xu, G.; Chen, L.; Li, Q. Association of Iron Metabolism Markers, Socioeconomic and Lifestyle Factors with Endometriosis: A Cross-Sectional Study. J. Trace Elem. Med. Biol. 2023, 78, 127175. [Google Scholar] [CrossRef]
- Burney, R.O.; Giudice, L.C. Pathogenesis and Pathophysiology of Endometriosis. Fertil. Steril. 2012, 98, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Koninckx, P.R.; Ussia, A.; Adamyan, L.; Wattiez, A.; Gomel, V.; Martin, D.C. Pathogenesis of Endometriosis: The Genetic/epigenetic Theory. Fertil. Steril. 2019, 111, 327–340. [Google Scholar] [CrossRef]
- Clower, L.; Fleshman, T.; Geldenhuys, W.J.; Santanam, N. Targeting Oxidative Stress Involved in Endometriosis and Its Pain. Biomolecules 2022, 12, 1055. [Google Scholar] [CrossRef]
- Li, Y.; Zeng, X.; Lu, D.; Yin, M.; Shan, M.; Gao, Y. Erastin Induces Ferroptosis via Ferroportin-Mediated Iron Accumulation in Endometriosis. Hum. Reprod. 2021, 36, 951–964. [Google Scholar] [CrossRef]
- Lobo, V.; Patil, A.; Phatak, A.; Chandra, N. Free Radicals, Antioxidants and Functional Foods: Impact on Human Health. Pharmacogn. Rev. 2010, 4, 118–126. [Google Scholar] [CrossRef]
- Sies, H. Oxidative Stress: A Concept in Redox Biology and Medicine. Redox Biol 2015, 4, 180–183. [Google Scholar] [CrossRef] [PubMed]
- Bisht, S.; Faiq, M.; Tolahunase, M.; Dada, R. Oxidative Stress and Male Infertility. Nat. Rev. Urol. 2017, 14, 470–485. [Google Scholar] [CrossRef]
- Soto-Heras, S.; Paramio, M.-T. Impact of Oxidative Stress on Oocyte Competence for in Vitro Embryo Production Programs. Res. Vet. Sci. 2020, 132, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Tang, J.; Wang, L.; Tan, F.; Song, H.; Zhou, J.; Li, F. Oxidative Stress in Oocyte Aging and Female Reproduction. J. Cell. Physiol. 2021, 236, 7966–7983. [Google Scholar] [CrossRef]
- Dutta, S.; Sengupta, P.; Slama, P.; Roychoudhury, S. Oxidative Stress, Testicular Inflammatory Pathways, and Male Reproduction. Int. J. Mol. Sci. 2021, 22, 10043. [Google Scholar] [CrossRef]
- Agarwal, A.; Aponte-Mellado, A.; Premkumar, B.J.; Shaman, A.; Gupta, S. The Effects of Oxidative Stress on Female Reproduction: A Review. Reprod. Biol. Endocrinol. 2012, 10, 49. [Google Scholar] [CrossRef] [PubMed]
- Assaf, L.; Eid, A.A.; Nassif, J. Role of AMPK/mTOR, Mitochondria, and ROS in the Pathogenesis of Endometriosis. Life Sci. 2022, 306, 120805. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, S.; Mateen, S.; Ahmad, R.; Moin, S. A Brief Insight into the Etiology, Genetics, and Immunology of Polycystic Ovarian Syndrome (PCOS). J. Assist. Reprod. Genet. 2022, 39, 2439–2473. [Google Scholar] [CrossRef] [PubMed]
- Rapa, S.F.; Di Iorio, B.R.; Campiglia, P.; Heidland, A.; Marzocco, S. Inflammation and Oxidative Stress in Chronic Kidney Disease-Potential Therapeutic Role of Minerals, Vitamins and Plant-Derived Metabolites. Int. J. Mol. Sci. 2019, 21, 263. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.N.; Siddiqui, S.A.; Uddin, M.G.; Ibrahim, M.; Uddin, S.M.N.; Adnan, M.T.; Rahaman, M.Z.; Kar, A.; Islam, M.S. Increased Oxidative Stress, Altered Trace Elements, and Macro-Minerals Are Associated with Female Obesity. Biol. Trace Elem. Res. 2020, 197, 384–393. [Google Scholar] [CrossRef]
- Samimi, M.; Pourhanifeh, M.H.; Mehdizadehkashi, A.; Eftekhar, T.; Asemi, Z. The Role of Inflammation, Oxidative Stress, Angiogenesis, and Apoptosis in the Pathophysiology of Endometriosis: Basic Science and New Insights Based on Gene Expression. J. Cell. Physiol. 2019, 234, 19384–19392. [Google Scholar] [CrossRef] [PubMed]
- Zejnullahu, V.A.; Zejnullahu, V.A.; Kosumi, E. The Role of Oxidative Stress in Patients with Recurrent Pregnancy Loss: A Review. Reprod. Health 2021, 18, 207. [Google Scholar] [CrossRef] [PubMed]
- Rudnicka, E.; Suchta, K.; Grymowicz, M.; Calik-Ksepka, A.; Smolarczyk, K.; Duszewska, A.M.; Smolarczyk, R.; Meczekalski, B. Chronic Low Grade Inflammation in Pathogenesis of PCOS. Int. J. Mol. Sci. 2021, 22, 3789. [Google Scholar] [CrossRef]
- Joo, E.H.; Kim, Y.R.; Kim, N.; Jung, J.E.; Han, S.H.; Cho, H.Y. Effect of Endogenic and Exogenic Oxidative Stress Triggers on Adverse Pregnancy Outcomes: Preeclampsia, Fetal Growth Restriction, Gestational Diabetes Mellitus and Preterm Birth. Int. J. Mol. Sci. 2021, 22, 10122. [Google Scholar] [CrossRef]
- Galaris, D.; Barbouti, A.; Pantopoulos, K. Iron Homeostasis and Oxidative Stress: An Intimate Relationship. Biochim. Biophys. Acta Mol. Cell Res. 2019, 1866, 118535. [Google Scholar] [CrossRef]
- Hariharan, S.; Dharmaraj, S. Selenium and Selenoproteins: It’s Role in Regulation of Inflammation. Inflammopharmacology 2020, 28, 667–695. [Google Scholar] [CrossRef]
- Powell, S.R. The Antioxidant Properties of Zinc. J. Nutr. 2000, 130, 1447S–1454S. [Google Scholar] [CrossRef]
- Maier, J.A.; Castiglioni, S.; Locatelli, L.; Zocchi, M.; Mazur, A. Magnesium and Inflammation: Advances and Perspectives. Semin. Cell Dev. Biol. 2021, 115, 37–44. [Google Scholar] [CrossRef]
- Khalid, H.; Hanif, M.; Hashmi, M.A.; Mahmood, T.; Ayub, K.; Monim-Ul-Mehboob, M. Copper Complexes of Bioactive Ligands with Superoxide Dismutase Activity. Mini Rev. Med. Chem. 2013, 13, 1944–1956. [Google Scholar] [CrossRef]
- Ferronato, G.A.; Alvarado-Rincón, J.A.; Maffi, A.S.; Barbosa, A.A.; Gasperin, B.G.; Schneider, A.; Mondadori, R.G.; Brauner, C.C.; Corrêa, M.N. Expression of Genes Associated with Fertility in the Uterus and Oviduct of Heifers Challenged with Lipopolysaccharide. Zygote 2022, 30, 584–587. [Google Scholar] [CrossRef]
- Choi, S.; Liu, X.; Pan, Z. Zinc Deficiency and Cellular Oxidative Stress: Prognostic Implications in Cardiovascular Diseases. Acta Pharmacol. Sin. 2018, 39, 1120–1132. [Google Scholar] [CrossRef] [PubMed]
- Prasad, A.S. Impact of the Discovery of Human Zinc Deficiency on Health. J. Trace Elem. Med. Biol. 2014, 28, 357–363. [Google Scholar] [CrossRef]
- Ota, E.; Mori, R.; Middleton, P.; Tobe-Gai, R.; Mahomed, K.; Miyazaki, C.; Bhutta, Z.A. Zinc Supplementation for Improving Pregnancy and Infant Outcome. Cochrane Database Syst. Rev. 2015, 2015, CD000230. [Google Scholar] [CrossRef] [PubMed]
- Gohari, H.; Khajavian, N.; Mahmoudian, A.; Bilandi, R.R. Copper and Zinc Deficiency to the Risk of Preterm Labor in Pregnant Women: A Case-Control Study. BMC Pregnancy Childbirth 2023, 23, 366. [Google Scholar] [CrossRef] [PubMed]
- Ménézo, Y.; Pluntz, L.; Chouteau, J.; Gurgan, T.; Demirol, A.; Dalleac, A.; Benkhalifa, M. Zinc Concentrations in Serum and Follicular Fluid during Ovarian Stimulation and Expression of Zn2+ Transporters in Human Oocytes and Cumulus Cells. Reprod. Biomed. Online 2011, 22, 647–652. [Google Scholar] [CrossRef]
- Falchuk, K.H.; Montorzi, M. Zinc Physiology and Biochemistry in Oocytes and Embryos. Biometals 2001, 14, 385–395. [Google Scholar] [CrossRef] [PubMed]
- Jose, N.; Elangovan, A.V.; Awachat, V.B.; Shet, D.; Ghosh, J.; David, C.G. Response of in Ovo Administration of Zinc on Egg Hatchability and Immune Response of Commercial Broiler Chicken. J. Anim. Physiol. Anim. Nutr. 2018, 102, 591–595. [Google Scholar] [CrossRef] [PubMed]
- Muraina, I.A.; Maret, W.; Bury, N.R.; Hogstrand, C. Hatching Gland Development and Hatching in Zebrafish Embryos: A Role for Zinc and Its Transporters Zip10 and Znt1a. Biochem. Biophys. Res. Commun. 2020, 528, 698–705. [Google Scholar] [CrossRef]
- Tian, X.; Anthony, K.; Neuberger, T.; Diaz, F.J. Preconception Zinc Deficiency Disrupts Postimplantation Fetal and Placental Development in Mice. Biol. Reprod. 2014, 90, 83. [Google Scholar] [CrossRef] [PubMed]
- Andrews, G.K.; Wang, H.; Dey, S.K.; Palmiter, R.D. Mouse Zinc Transporter 1 Gene Provides an Essential Function during Early Embryonic Development. Genesis 2004, 40, 74–81. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.L.; Grieger, J.A.; Bianco-Miotto, T.; Roberts, C.T. Association between Maternal Zinc Status, Dietary Zinc Intake and Pregnancy Complications: A Systematic Review. Nutrients 2016, 8, 641. [Google Scholar] [CrossRef] [PubMed]
- Wessels, I.; Maywald, M.; Rink, L. Zinc as a Gatekeeper of Immune Function. Nutrients 2017, 9, 1286. [Google Scholar] [CrossRef] [PubMed]
- Eide, D.J. The Oxidative Stress of Zinc Deficiency. Metallomics 2011, 3, 1124–1129. [Google Scholar] [CrossRef] [PubMed]
- Messalli, E.M.; Schettino, M.T.; Mainini, G.; Ercolano, S.; Fuschillo, G.; Falcone, F.; Esposito, E.; Di Donna, M.C.; De Franciscis, P.; Torella, M. The Possible Role of Zinc in the Etiopathogenesis of Endometriosis. Clin. Exp. Obstet. Gynecol. 2014, 41, 541–546. [Google Scholar] [CrossRef]
- Mier-Cabrera, J.; Aburto-Soto, T.; Burrola-Méndez, S.; Jiménez-Zamudio, L.; Tolentino, M.C.; Casanueva, E.; Hernández-Guerrero, C. Women with Endometriosis Improved Their Peripheral Antioxidant Markers after the Application of a High Antioxidant Diet. Reprod. Biol. Endocrinol. 2009, 7, 54. [Google Scholar] [CrossRef]
- Bonaventura, P.; Benedetti, G.; Albarède, F.; Miossec, P. Zinc and Its Role in Immunity and Inflammation. Autoimmun. Rev. 2015, 14, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Maret, W.; Sandstead, H.H. Zinc Requirements and the Risks and Benefits of Zinc Supplementation. J. Trace Elem. Med. Biol. 2006, 20, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Hao, Q.; Maret, W. Imbalance between pro-Oxidant and pro-Antioxidant Functions of Zinc in Disease. J. Alzheimers Dis. 2005, 8, 161–170; discussion 209–215. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.R. Critical Role of Zinc as Either an Antioxidant or a Prooxidant in Cellular Systems. Oxid. Med. Cell. Longev. 2018, 2018, 9156285. [Google Scholar] [CrossRef] [PubMed]
- Ahsan, U.; Kamran, Z.; Raza, I.; Ahmad, S.; Babar, W.; Riaz, M.H.; Iqbal, Z. Role of Selenium in Male Reproduction—A Review. Anim. Reprod. Sci. 2014, 146, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Boitani, C.; Puglisi, R. Selenium, a Key Element in Spermatogenesis and Male Fertility. Adv. Exp. Med. Biol. 2008, 636, 65–73. [Google Scholar] [PubMed]
- Singh, A.K.; Chattopadhyay, R.; Chakravarty, B.; Chaudhury, K. Markers of Oxidative Stress in Follicular Fluid of Women with Endometriosis and Tubal Infertility Undergoing IVF. Reprod. Toxicol. 2013, 42, 116–124. [Google Scholar] [CrossRef]
- Adeniran, S.O.; Zheng, P.; Feng, R.; Adegoke, E.O.; Huang, F.; Ma, M.; Wang, Z.; Ifarajimi, O.O.; Li, X.; Zhang, G. The Antioxidant Role of Selenium via GPx1 and GPx4 in LPS-Induced Oxidative Stress in Bovine Endometrial Cells. Biol. Trace Elem. Res. 2022, 200, 1140–1155. [Google Scholar] [CrossRef] [PubMed]
- Crites, B.R. The Effects of Form of Selenium on the Bovine Corpus Luteum, Uterine Endometrium, and Development of the Conceptus. Ph.D. Thesis, University of Kentucky, Lexington, KY, USA, 2021. [Google Scholar]
- Jankowski, C.S.R.; Rabinowitz, J.D. Selenium Modulates Cancer Cell Response to Pharmacologic Ascorbate. Cancer Res. 2022, 82, 3486–3498. [Google Scholar] [CrossRef]
- Selenium: An Essential Element for Glutathione Peroxidase Activity. Nutr. Rev. 1973, 31, 289–291.
- Yan, F.; Zhao, Q.; Li, Y.; Zheng, Z.; Kong, X.; Shu, C.; Liu, Y.; Shi, Y. The Role of Oxidative Stress in Ovarian Aging: A Review. J. Ovarian Res. 2022, 15, 100. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Luderer, U. Oxidative Damage Increases and Antioxidant Gene Expression Decreases with Aging in the Mouse Ovary. Biol. Reprod. 2011, 84, 775–782. [Google Scholar] [CrossRef] [PubMed]
- Timóteo-Ferreira, F.; Abreu, D.; Mendes, S.; Matos, L.; Rodrigues, A.R.; Almeida, H.; Silva, E. Redox Imbalance in Age-Related Ovarian Dysfunction and Perspectives for Its Prevention. Ageing Res. Rev. 2021, 68, 101345. [Google Scholar] [CrossRef] [PubMed]
- Adeoye, O.; Olawumi, J.; Opeyemi, A.; Christiania, O. Review on the Role of Glutathione on Oxidative Stress and Infertility. JBRA Assist. Reprod. 2018, 22, 61–66. [Google Scholar] [CrossRef] [PubMed]
- Grazul-Bilska, A.T.; Caton, J.S.; Arndt, W.; Burchill, K.; Thorson, C.; Borowczyk, E.; Bilski, J.J.; Redmer, D.A.; Reynolds, L.P.; Vonnahme, K.A. Cellular Proliferation and Vascularization in Ovine Fetal Ovaries: Effects of Undernutrition and Selenium in Maternal Diet. Reproduction 2009, 137, 699–707. [Google Scholar] [CrossRef] [PubMed]
- Basini, G.; Tamanini, C. Selenium Stimulates Estradiol Production in Bovine Granulosa Cells: Possible Involvement of Nitric Oxide. Domest. Anim. Endocrinol. 2000, 18, 1–17. [Google Scholar] [CrossRef]
- Ceko, M.J.; Hummitzsch, K.; Hatzirodos, N.; Bonner, W.M.; Aitken, J.B.; Russell, D.L.; Lane, M.; Rodgers, R.J.; Harris, H.H. X-Ray Fluorescence Imaging and Other Analyses Identify Selenium and GPX1 as Important in Female Reproductive Function. Metallomics 2015, 7, 71–82. [Google Scholar] [CrossRef]
- Pieczyńska, J.; Grajeta, H. The Role of Selenium in Human Conception and Pregnancy. J. Trace Elem. Med. Biol. 2015, 29, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Hernández Guerrero, C.A.; Bujalil Montenegro, L.; de la Jara Díaz, J.; Mier Cabrera, J.; Bouchán Valencia, P. Endometriosis and deficient intake of antioxidants molecules related to peripheral and peritoneal oxidative stress. Ginecol. Obstet. Mex. 2006, 74, 20–28. [Google Scholar]
- Morgia, G.; Cimino, S.; Favilla, V.; Russo, G.I.; Squadrito, F.; Mucciardi, G.; Masieri, L.; Minutoli, L.; Grosso, G.; Castelli, T. Effects of Serenoa Repens, Selenium and Lycopene (Profluss®) on Chronic Inflammation Associated with Benign Prostatic Hyperplasia: Results of “FLOG” (Flogosis and Profluss in Prostatic and Genital Disease), a Multicentre Italian Study. Int. Braz. J. Urol. 2013, 39, 214–221. [Google Scholar] [CrossRef]
- Harris, E.D. Copper as a Cofactor and Regulator of Copper,zinc Superoxide Dismutase. J. Nutr. 1992, 122, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Solier, S.; Müller, S.; Cañeque, T.; Versini, A.; Mansart, A.; Sindikubwabo, F.; Baron, L.; Emam, L.; Gestraud, P.; Pantoș, G.D.; et al. A Druggable Copper-Signalling Pathway That Drives Inflammation. Nature 2023, 617, 386–394. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Kang, Y.; Chang, Q.; Zhang, B.; Liu, X.; Zeng, L.; Yan, H.; Dang, S. Maternal Zinc, Copper, and Selenium Intakes during Pregnancy and Congenital Heart Defects. Nutrients 2022, 14, 1055. [Google Scholar] [CrossRef] [PubMed]
- Yang, D.; Xiao, P.; Qiu, B.; Yu, H.-F.; Teng, C.-B. Copper Chaperone Antioxidant 1: Multiple Roles and a Potential Therapeutic Target. J. Mol. Med. 2023, 101, 527–542. [Google Scholar] [CrossRef] [PubMed]
- Michaluk, A.; Kochman, K. Involvement of Copper in Female Reproduction. Reprod. Biol. 2007, 7, 193–205. [Google Scholar] [PubMed]
- Gao, G.; Yi, J.; Zhang, M.; Xiong, J.; Geng, L.; Mu, C.; Yang, L. Effects of Iron and Copper in Culture Medium on Bovine Oocyte Maturation, Preimplantation Embryo Development, and Apoptosis of Blastocysts In Vitro. J. Reprod. Dev. 2007, 53, 777–784. [Google Scholar] [CrossRef] [PubMed]
- Choi, H.; Lee, J.; Yoon, J.D.; Hwang, S.-U.; Cai, L.; Kim, M.; Kim, G.; Oh, D.; Kim, E.; Hyun, S.-H. The Effect of Copper Supplementation on in Vitro Maturation of Porcine Cumulus-Oocyte Complexes and Subsequent Developmental Competence after Parthenogenetic Activation. Theriogenology 2021, 164, 84–92. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Glubb, D.M.; O’Mara, T.A. Dietary Factors and Endometrial Cancer Risk: A Mendelian Randomization Study. Nutrients 2023, 15, 603. [Google Scholar] [CrossRef] [PubMed]
- Ho, Y.S.; Gargano, M.; Cao, J.; Bronson, R.T.; Heimler, I.; Hutz, R.J. Reduced Fertility in Female Mice Lacking Copper-Zinc Superoxide Dismutase. J. Biol. Chem. 1998, 273, 7765–7769. [Google Scholar] [CrossRef] [PubMed]
- Roychoudhury, S.; Nath, S.; Massanyi, P.; Stawarz, R.; Kacaniova, M.; Kolesarova, A. Copper-Induced Changes in Reproductive Functions: In Vivo and in Vitro Effects. Physiol. Res. 2016, 65, 11–22. [Google Scholar] [CrossRef]
- Galaris, D.; Pantopoulos, K. Oxidative Stress and Iron Homeostasis: Mechanistic and Health Aspects. Crit. Rev. Clin. Lab. Sci. 2008, 45, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Kawabata, T. Iron-Induced Oxidative Stress in Human Diseases. Cells 2022, 11, 2152. [Google Scholar] [CrossRef] [PubMed]
- Golfeyz, S.; Lewis, S.; Weisberg, I.S. Hemochromatosis: Pathophysiology, Evaluation, and Management of Hepatic Iron Overload with a Focus on MRI. Expert Rev. Gastroenterol. Hepatol. 2018, 12, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Sun, K.; Guo, Z.; Hou, L.; Xu, J.; Du, T.; Xu, T.; Guo, F. Iron Homeostasis in Arthropathies: From Pathogenesis to Therapeutic Potential. Ageing Res. Rev. 2021, 72, 101481. [Google Scholar] [CrossRef] [PubMed]
- Gattermann, N.; Muckenthaler, M.U.; Kulozik, A.E.; Metzgeroth, G.; Hastka, J. The Evaluation of Iron Deficiency and Iron Overload. Dtsch. Arztebl. Int. 2021, 118, 847–856. [Google Scholar] [CrossRef] [PubMed]
- Camaioni, A.; Ucci, M.A.; Campagnolo, L.; De Felici, M.; Klinger, F.G. Italian Society of Embryology, Reproduction and Research (SIERR) The Process of Ovarian Aging: It Is Not Just about Oocytes and Granulosa Cells. J. Assist. Reprod. Genet. 2022, 39, 783–792. [Google Scholar] [CrossRef] [PubMed]
- Chiang, J.L.; Shukla, P.; Pagidas, K.; Ahmed, N.S.; Karri, S.; Gunn, D.D.; Hurd, W.W.; Singh, K.K. Mitochondria in Ovarian Aging and Reproductive Longevity. Ageing Res. Rev. 2020, 63, 101168. [Google Scholar] [CrossRef] [PubMed]
- Broekmans, F.J.; Soules, M.R.; Fauser, B.C. Ovarian Aging: Mechanisms and Clinical Consequences. Endocr. Rev. 2009, 30, 465–493. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Nan, B.; Kong, S.; Harlow, S. Changes in Iron Measures over Menopause and Associations with Insulin Resistance. J. Women’s Health 2012, 21, 872–877. [Google Scholar] [CrossRef]
- Liu, M.; Wu, K.; Wu, Y. The Emerging Role of Ferroptosis in Female Reproductive Disorders. Biomed. Pharmacother. 2023, 166, 115415. [Google Scholar] [CrossRef]
- Li, X.; Duan, X.; Tan, D.; Zhang, B.; Xu, A.; Qiu, N.; Chen, Z. Iron Deficiency and Overload in Men and Woman of Reproductive Age, and Pregnant Women. Reprod. Toxicol. 2023, 118, 108381. [Google Scholar] [CrossRef] [PubMed]
- Fanni, D.; Gerosa, C.; Nurchi, V.M.; Manchia, M.; Saba, L.; Coghe, F.; Crisponi, G.; Gibo, Y.; Van Eyken, P.; Fanos, V.; et al. The Role of Magnesium in Pregnancy and in Fetal Programming of Adult Diseases. Biol. Trace Elem. Res. 2021, 199, 3647–3657. [Google Scholar] [CrossRef] [PubMed]
- Hartwig, A. Role of Magnesium in Genomic Stability. Mutat. Res. 2001, 475, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Zheltova, A.A.; Kharitonova, M.V.; Iezhitsa, I.N.; Spasov, A.A. Magnesium Deficiency and Oxidative Stress: An Update. Biomedicine 2016, 6, 20. [Google Scholar] [CrossRef] [PubMed]
- Mousavi, R.; Alizadeh, M.; Asghari Jafarabadi, M.; Heidari, L.; Nikbakht, R.; Babaahmadi Rezaei, H.; Karandish, M. Effects of Melatonin And/or Magnesium Supplementation on Biomarkers of Inflammation and Oxidative Stress in Women with Polycystic Ovary Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Biol. Trace Elem. Res. 2022, 200, 1010–1019. [Google Scholar] [CrossRef]
- Hsu, J.M.; Rubenstein, B.; Paleker, A.G. Role of Magnesium in Glutathione Metabolism of Rat Erythrocytes. J. Nutr. 1982, 112, 488–496. [Google Scholar] [CrossRef] [PubMed]
- Dickens, B.F.; Weglicki, W.B.; Li, Y.S.; Mak, I.T. Magnesium Deficiency in Vitro Enhances Free Radical-Induced Intracellular Oxidation and Cytotoxicity in Endothelial Cells. FEBS Lett. 1992, 311, 187–191. [Google Scholar] [CrossRef]
- Zhang, Y.; Davies, L.R.; Martin, S.M.; Bawaney, I.M.; Buettner, G.R.; Kerber, R.E. Magnesium Reduces Free Radical Concentration and Preserves Left Ventricular Function after Direct Current Shocks. Resuscitation 2003, 56, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Garcia, L.A.; DeJong, S.C.; Martin, S.M.; Smith, R.S.; Buettner, G.R.; Kerber, R.E. Magnesium Reduces Free Radicals in an in Vivo Coronary Occlusion-Reperfusion Model. J. Am. Coll. Cardiol. 1998, 32, 536–539. [Google Scholar] [CrossRef]
- Morais, J.B.S.; Severo, J.S.; Santos, L.R.D.; de Sousa Melo, S.R.; de Oliveira Santos, R.; de Oliveira, A.R.S.; Cruz, K.J.C.; do Nascimento Marreiro, D. Role of Magnesium in Oxidative Stress in Individuals with Obesity. Biol. Trace Elem. Res. 2017, 176, 20–26. [Google Scholar] [CrossRef]
- Zarean, E.; Tarjan, A. Effect of Magnesium Supplement on Pregnancy Outcomes: A Randomized Control Trial. Adv. Biomed. Res. 2017, 6, 109. [Google Scholar]
- Grossi, E.; Castiglioni, S.; Moscheni, C.; Antonazzo, P.; Cetin, I.; Savasi, V.M. Serum Magnesium and Calcium Levels in Infertile Women during a Cycle of Reproductive Assistance. Magnes. Res. 2017, 30, 35–41. [Google Scholar] [CrossRef] [PubMed]
- Makrides, M.; Crosby, D.D.; Bain, E.; Crowther, C.A. Magnesium Supplementation in Pregnancy. Cochrane Database Syst. Rev. 2014, 2014, CD000937. [Google Scholar] [CrossRef] [PubMed]
- Gao, W.; Feng, F.; Ma, X.; Zhang, R.; Li, L.; Yue, F.; Lv, M.; Liu, L. Progress of Oxidative Stress in Endometrium Decidualization. J. Obstet. Gynaecol. 2022, 42, 3429–3434. [Google Scholar] [CrossRef]
- Li, W.; Liu, C.; Yang, Q.; Zhou, Y.; Liu, M.; Shan, H. Oxidative Stress and Antioxidant Imbalance in Ovulation Disorder in Patients with Polycystic Ovary Syndrome. Front. Nutr. 2022, 9, 1018674. [Google Scholar] [CrossRef]
- Yuan, J.; Yu, Y.; Zhu, T.; Lin, X.; Jing, X.; Zhang, J. Oral Magnesium Supplementation for the Prevention of Preeclampsia: A Meta-Analysis or Randomized Controlled Trials. Biol. Trace Elem. Res. 2022, 200, 3572–3581. [Google Scholar] [CrossRef]
- Pereira, A.C.; Martel, F. Oxidative Stress in Pregnancy and Fertility Pathologies. Cell Biol. Toxicol. 2014, 30, 301–312. [Google Scholar] [CrossRef]
- Studer, J.M.; Schweer, W.P.; Gabler, N.K.; Ross, J.W. Functions of Manganese in Reproduction. Anim. Reprod. Sci. 2022, 238, 106924. [Google Scholar] [CrossRef]
- Chen, P.; Bornhorst, J.; Aschner, M. Manganese Metabolism in Humans. Front. Biosci. 2018, 23, 1655–1679. [Google Scholar] [CrossRef]
- Golara, A.; Kozłowski, M.; Guzik, P.; Kwiatkowski, S.; Cymbaluk-Płoska, A. The Role of Selenium and Manganese in the Formation, Diagnosis and Treatment of Cervical, Endometrial and Ovarian Cancer. Int. J. Mol. Sci. 2023, 24, 10887. [Google Scholar] [CrossRef]
- Tholin, K.; Palm, R.; Hallmans, G.; Sandström, B. Manganese Status during Pregnancy. Ann. N. Y. Acad. Sci. 1993, 678, 359–360. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Hivert, M.-F.; Rifas-Shiman, S.L.; Rahman, M.L.; Oken, E.; Cardenas, A.; Mueller, N.T. Prospective Association Between Manganese in Early Pregnancy and the Risk of Preeclampsia. Epidemiology 2020, 31, 677–680. [Google Scholar] [CrossRef] [PubMed]
- O’Neal, S.L.; Zheng, W. Manganese Toxicity Upon Overexposure: A Decade in Review. Curr. Environ. Health Rep. 2015, 2, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Ishikawa, M. Oxygen radicals-superoxide dismutase system and reproduction medicine. Nihon Sanka Fujinka Gakkai Zasshi 1993, 45, 842–848. [Google Scholar] [PubMed]
- Sugino, N.; Takiguchi, S.; Kashida, S.; Karube, A.; Nakamura, Y.; Kato, H. Superoxide Dismutase Expression in the Human Corpus Luteum during the Menstrual Cycle and in Early Pregnancy. Mol. Hum. Reprod. 2000, 6, 19–25. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.S.; Joo, B.S.; Na, Y.J.; Yoon, M.S.; Choi, O.H.; Kim, W.W. Relationships between Concentrations of Tumor Necrosis Factor-Alpha and Nitric Oxide in Follicular Fluid and Oocyte Quality. J. Assist. Reprod. Genet. 2000, 17, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Holden, E.C.; Dodge, L.E.; Sneeringer, R.; Moragianni, V.A.; Penzias, A.S.; Hacker, M.R. Thicker Endometrial Linings Are Associated with Better IVF Outcomes: A Cohort of 6331 Women. Hum. Fertil. 2018, 21, 288–293. [Google Scholar] [CrossRef]
- Blanco-Breindel, M.F.; Singh, M.; Kahn, J. Endometrial Receptivity. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Critchley, H.O.D.; Maybin, J.A.; Armstrong, G.M.; Williams, A.R.W. Physiology of the Endometrium and Regulation of Menstruation. Physiol. Rev. 2020, 100, 1149–1179. [Google Scholar] [CrossRef]
- Haas, J.; Casper, R.F. Observations on Clinical Assessment of Endometrial Receptivity. Fertil. Steril. 2022, 118, 828–831. [Google Scholar] [CrossRef]
- Bavan, B.; Gardner, R.M.; Zhang, W.Y.; Aghajanova, L. The Effect of Human Growth Hormone on Endometrial Growth in Controlled Ovarian Hyperstimulation Cycles. J. Pers. Med. 2022, 12, 1991. [Google Scholar] [CrossRef]
- Navot, D.; Scott, R.T.; Droesch, K.; Veeck, L.L.; Liu, H.C.; Rosenwaks, Z. The Window of Embryo Transfer and the Efficiency of Human Conception in Vitro. Fertil. Steril. 1991, 55, 114–118. [Google Scholar] [CrossRef] [PubMed]
- Muter, J.; Lynch, V.J.; McCoy, R.C.; Brosens, J.J. Human Embryo Implantation. Development 2023, 150, dev201507. [Google Scholar] [CrossRef] [PubMed]
- Norwitz, E.R.; Schust, D.J.; Fisher, S.J. Implantation and the Survival of Early Pregnancy. N. Engl. J. Med. 2001, 345, 1400–1408. [Google Scholar] [CrossRef] [PubMed]
- Shafei, R.A.; Syrkasheva, A.G.; Romanov, A.Y.; Makarova, N.P.; Dolgushina, N.V.; Semenova, M.L. Blastocyst Hatching in Humans. Ontogenez 2017, 48, 8–20. [Google Scholar] [CrossRef] [PubMed]
- Gauster, M.; Moser, G.; Wernitznig, S.; Kupper, N.; Huppertz, B. Early Human Trophoblast Development: From Morphology to Function. Cell. Mol. Life Sci. 2022, 79, 345. [Google Scholar] [CrossRef] [PubMed]
- Brosens, J.J.; Salker, M.S.; Teklenburg, G.; Nautiyal, J.; Salter, S.; Lucas, E.S.; Steel, J.H.; Christian, M.; Chan, Y.-W.; Boomsma, C.M.; et al. Uterine Selection of Human Embryos at Implantation. Sci. Rep. 2014, 4, 3894. [Google Scholar] [CrossRef] [PubMed]
- Scholl, T.O. Iron Status during Pregnancy: Setting the Stage for Mother and Infant. Am. J. Clin. Nutr. 2005, 81, 1218S–1222S. [Google Scholar] [CrossRef] [PubMed]
- Zachara, B.A.; Dobrzyński, W.; Trafikowska, U.; Szymański, W. Blood Selenium and Glutathione Peroxidases in Miscarriage. BJOG 2001, 108, 244–247. [Google Scholar] [PubMed]
- Pandur, E.; Pap, R.; Jánosa, G.; Horváth, A.; Sipos, K. Fractalkine Improves the Expression of Endometrium Receptivity-Related Genes and Proteins at Desferrioxamine-Induced Iron Deficiency in HEC-1A Cells. Int. J. Mol. Sci. 2023, 24, 7924. [Google Scholar] [CrossRef]
- Pandur, E.; Pap, R.; Montskó, G.; Jánosa, G.; Sipos, K.; Kovács, G.L. Fractalkine Enhances Endometrial Receptivity and Activates Iron Transport towards Trophoblast Cells in an in Vitro Co-Culture System of HEC-1A and JEG-3 Cells. Exp. Cell Res. 2021, 403, 112583. [Google Scholar] [CrossRef]
- Prasad, A.S. Zinc: An Overview. Nutrition 1995, 11, 93–99. [Google Scholar] [PubMed]
- Lu, X.; Zhang, Q.; Xu, L.; Lin, X.; Fu, J.; Wang, X.; Liu, Y.; Lin, Y.; Li, B.; Wang, R.; et al. Zinc Is Essential for the Transcription Function of the PGC-1α/Nrf2 Signaling Pathway in Human Primary Endometrial Stromal Cells. Am. J. Physiol.-Cell Physiol. 2020, 318, C640–C648. [Google Scholar] [CrossRef] [PubMed]
- Grieger, J.A.; Grzeskowiak, L.E.; Wilson, R.L.; Bianco-Miotto, T.; Leemaqz, S.Y.; Jankovic-Karasoulos, T.; Perkins, A.V.; Norman, R.J.; Dekker, G.A.; Roberts, C.T. Maternal Selenium, Copper and Zinc Concentrations in Early Pregnancy, and the Association with Fertility. Nutrients 2019, 11, 1609. [Google Scholar] [CrossRef] [PubMed]
- Lai, G.-L.; Yeh, C.-C.; Yeh, C.-Y.; Chen, R.-Y.; Fu, C.-L.; Chen, C.-H.; Tzeng, C.-R. Decreased Zinc and Increased Lead Blood Levels Are Associated with Endometriosis in Asian Women. Reprod. Toxicol. 2017, 74, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Jang, H.; Yoo, I.; Han, J.; Jung, W.; Ka, H. Unique Epithelial Expression of S100A Calcium Binding Protein A7A in the Endometrium at Conceptus Implantation in Pigs. Asian-Australas. J. Anim. Sci. 2019, 32, 1355–1362. [Google Scholar] [CrossRef]
- Choi, Y.; Jang, H.; Seo, H.; Yoo, I.; Han, J.; Kim, M.; Lee, S.; Ka, H. Changes in Calcium Levels in the Endometrium throughout Pregnancy and the Role of Calcium on Endometrial Gene Expression at the Time of Conceptus Implantation in Pigs. Mol. Reprod. Dev. 2019, 86, 883–895. [Google Scholar] [CrossRef] [PubMed]
- Li, G.; Han, N.; Yang, H.; Wang, L.; Lin, X.; Diao, S.; Du, J.; Dong, R.; Wang, S.; Fan, Z. Homeobox C10 Inhibits the Osteogenic Differentiation Potential of Mesenchymal Stem Cells. Connect. Tissue Res. 2018, 59, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Metcalf, D. The Leukemia Inhibitory Factor (LIF). Stem Cells 1996, 9, 95–108. [Google Scholar] [CrossRef] [PubMed]
- Bi, Y.; Huang, W.; Yuan, L.; Chen, S.; Liao, S.; Fu, X.; Liu, B.; Yang, Y. HOXA10 Improves Endometrial Receptivity by Upregulating E-Cadherin. Biol. Reprod. 2022, 106, 992–999. [Google Scholar] [CrossRef]
- Taylor, H.S.; Vanden Heuvel, G.B.; Igarashi, P. A Conserved Hox Axis in the Mouse and Human Female Reproductive System: Late Establishment and Persistent Adult Expression of the Hoxa Cluster Genes. Biol. Reprod. 1997, 57, 1338–1345. [Google Scholar] [CrossRef]
- Du, H.; Taylor, H.S. The Role of Hox Genes in Female Reproductive Tract Development, Adult Function, and Fertility. Cold Spring Harb. Perspect. Med. 2015, 6, a023002. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Chen, X.; Saravelos, S.H.; Liu, Y.; Huang, J.; Zhang, J.; Li, T.C. HOXA-10 and E-Cadherin Expression in the Endometrium of Women with Recurrent Implantation Failure and Recurrent Miscarriage. Fertil. Steril. 2017, 107, 136–143.e2. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, M.M.A.; Nafady, A.; Taha, S.A.M.; El-Din, A.M.G.; Ali, A.E.-N.A.E.-G. Leukemia Inhibitory Factor a Marker of Implantation Success in Unexplained Infertility: A Randomized Controlled Trial. Clin. Lab. 2022, 68, 2454. [Google Scholar] [CrossRef]
- Choi, K.C.; An, B.S.; Yang, H.; Jeung, E.B. Regulation and Molecular Mechanisms of Calcium Transport Genes: Do They Play a Role in Calcium Transport in the Uterine Endometrium? J. Physiol. Pharmacol. 2011, 62, 499–504. [Google Scholar]
- Nakamura, H.; Kimura, T.; Ogita, K.; Nakamura, T.; Takemura, M.; Shimoya, K.; Koyama, S.; Tsujie, T.; Koyama, M.; Murata, Y. NF-kappaB Activation at Implantation Window of the Mouse Uterus. Am. J. Reprod. Immunol. 2004, 51, 16–21. [Google Scholar] [CrossRef]
- Omer, F. Department of Reproduction and obstetrics, Faculty of Veterinary Medicine, University of Khartoum, Shambat, Sudan Intrauterine Infusion of Lugol’s Iodine Improves the Reproductive Traits of Postpartum Infected Dairy Cows. IOSR J. Agric. Vet. Sci. 2013, 5, 89–94. [Google Scholar] [CrossRef]
- Yoshida, R.; Kitahara, G.; Osawa, T. Intrauterine Infusion of Povidone-Iodine: Its Effect on the Endometrium and Subsequent Fertility in Postpartum Dairy Cows. J. Vet. Med. Sci. 2020, 82, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Mido, S.; Murata, N.; Rawy, M.S.; Kitahara, G.; Osawa, T. Effects of Intrauterine Infusion of Povidone-Iodine on Endometrial Cytology and Bacteriology in Dairy Cows with Clinical Endometritis. J. Vet. Med. Sci. 2016, 78, 551–556. [Google Scholar] [CrossRef]
- Johnson, N.P.; Bhattu, S.; Wagner, A.; Blake, D.A.; Chamley, L.W. Lipiodol Alters Murine Uterine Dendritic Cell Populations: A Potential Mechanism for the Fertility-Enhancing Effect of Lipiodol. Fertil. Steril. 2005, 83, 1814–1821. [Google Scholar] [CrossRef]
- Johnson, N.P.; Kwok, R.; Stewart, A.W.; Saththianathan, M.; Hadden, W.E.; Chamley, L.W. Lipiodol Fertility Enhancement: Two-Year Follow-up of a Randomized Trial Suggests a Transient Benefit in Endometriosis, but a Sustained Benefit in Unexplained Infertility. Hum. Reprod. 2007, 22, 2857–2862. [Google Scholar] [CrossRef]
- van Dyk, E.; Lange, A.L. The detrimental effect of iodine as an intra-uterine instillation in mares. J. S. Afr. Vet. Assoc. 1986, 57, 205–210. [Google Scholar] [PubMed]
- Wang, S.; Bu, Y.; Shao, Q.; Cai, Y.; Sun, D.; Fan, L. A Cohort Study on the Effects of Maternal High Serum Iodine Status During Pregnancy on Infants in Terms of Iodine Status and Intellectual, Motor, and Physical Development. Biol. Trace Elem. Res. 2023, 202, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Pearce, E.N.; Lazarus, J.H.; Moreno-Reyes, R.; Zimmermann, M.B. Consequences of Iodine Deficiency and Excess in Pregnant Women: An Overview of Current Knowns and Unknowns. Am. J. Clin. Nutr. 2016, 104 (Suppl. S3), 918S–923S. [Google Scholar] [CrossRef] [PubMed]
- Kuehn, B. Iodine Deficiency May Impair Fertility. JAMA 2018, 319, 760. [Google Scholar] [CrossRef] [PubMed]
- Seelig, M.S. Interrelationship of Magnesium and Estrogen in Cardiovascular and Bone Disorders, Eclampsia, Migraine and Premenstrual Syndrome. J. Am. Coll. Nutr. 1993, 12, 442–458. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-C.; Yang, P.-K.; Chen, L.-C.; Cheong, M.-L.; Tsai, Y.-L.; Tsai, M.-S. Associations between Gene Expression of Magnesium Transporters and Glucose Metabolism in Pregnancy. J. Formos. Med. Assoc. 2022, 121, 1231–1237. [Google Scholar] [CrossRef] [PubMed]
- Gholizadeh-Moghaddam, M.; Ghasemi-Tehrani, H.; Askari, G.; Jaripur, M.; Clark, C.C.T.; Rouhani, M.H. Effect of Magnesium Supplementation in Improving Hyperandrogenism, Hirsutism, and Sleep Quality in Women with Polycystic Ovary Syndrome: A Randomized, Placebo-Controlled Clinical Trial. Health Sci. Rep. 2023, 6, e1013. [Google Scholar] [CrossRef]
- Guerrero-Romero, F.; Rodríguez-Morán, M. Hypomagnesemia, Oxidative Stress, Inflammation, and Metabolic Syndrome. Diabetes Metab. Res. Rev. 2006, 22, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Aal-Hamad, A.H.; Al-Alawi, A.M.; Kashoub, M.S.; Falhammar, H. Hypermagnesemia in Clinical Practice. Medicina 2023, 59, 1190. [Google Scholar] [CrossRef]
- Simpson, W.G.; Vernon, M.E.; Jones, H.M.; Rush, M.E. The Role of Calcium in Gonadotropin-Releasing Hormone Induction of Follicle-Stimulating Hormone Release by the Pituitary Gonadotrope. Endocr. Res. 1989, 15, 355–373. [Google Scholar] [CrossRef]
- Murugesu, S.; Saso, S.; Jones, B.P.; Bracewell-Milnes, T.; Athanasiou, T.; Mania, A.; Serhal, P.; Ben-Nagi, J. Does the Use of Calcium Ionophore during Artificial Oocyte Activation Demonstrate an Effect on Pregnancy Rate? A Meta-Analysis. Fertil. Steril. 2017, 108, 468–482.e3. [Google Scholar] [CrossRef] [PubMed]
- Shoham, Z.; Homburg, R.; Jacobs, H.S. Induction of Ovulation with Pulsatile GnRH. Baillieres. Clin. Obstet. Gynaecol. 1990, 4, 589–608. [Google Scholar] [CrossRef] [PubMed]
- Zimmermann, M.B.; Boelaert, K. Iodine Deficiency and Thyroid Disorders. Lancet Diabetes Endocrinol. 2015, 3, 286–295. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Zinc. EFSA J. 2014, 12, 3844. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Iron. EFSA J. 2015, 13, 4254. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Selenium. EFSA J. 2014, 12, 3846. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Calcium. EFSA J. 2015, 13, 4101. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Magnesium. EFSA J. 2015, 13, 4186. [Google Scholar]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Iodine. EFSA J. 2014, 12, 3660. [Google Scholar] [CrossRef]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Copper. EFSA J. 2015, 13, 4253. [Google Scholar] [CrossRef]
- Institute of Medicine; Food and Nutrition Board; Standing Committee on the Scientific Evaluation of Dietary Reference Intakes; Subcommittee of Interpretation and Uses of Dietary Reference Intakes; Subcommittee on Upper Reference Levels of Nutrients; Panel on Micronutrients. Dietary Reference Intakes for Vitamin A, Vitamin K, Arsenic, Boron, Chromium, Copper, Iodine, Iron, Manganese, Molybdenum, Nickel, Silicon, Vanadium, and Zinc; National Academies Press: Cambridge, MA, USA, 2002; ISBN 978-0-30-907279-3. [Google Scholar]
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific Opinion on Dietary Reference Values for Manganese. EFSA J. 2013, 11, 3419. [Google Scholar] [CrossRef]
- Obiagwu, H.I.; Eleje, G.U.; Obiechina, N.J.A.; Nwosu, B.O.; Udigwe, G.O.; Ikechebelu, J.I.; Ugboaja, J.O.; Okoro, C.C.; Okonkwo, I.O.; Okwuosa, A.O.; et al. Efficacy of Zinc Supplementation for the Treatment of Dysmenorrhoea: A Double-Blind Randomised Controlled Trial. J. Int. Med. Res. 2023, 51, 3000605231171489. [Google Scholar] [CrossRef]
- Jamilian, M.; Foroozanfard, F.; Bahmani, F.; Talaee, R.; Monavari, M.; Asemi, Z. Effects of Zinc Supplementation on Endocrine Outcomes in Women with Polycystic Ovary Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Biol. Trace Elem. Res. 2016, 170, 271–278. [Google Scholar] [CrossRef]
- Afshar Ebrahimi, F.; Foroozanfard, F.; Aghadavod, E.; Bahmani, F.; Asemi, Z. The Effects of Magnesium and Zinc Co-Supplementation on Biomarkers of Inflammation and Oxidative Stress, and Gene Expression Related to Inflammation in Polycystic Ovary Syndrome: A Randomized Controlled Clinical Trial. Biol. Trace Elem. Res. 2018, 184, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Jamilian, M.; Mirhosseini, N.; Eslahi, M.; Bahmani, F.; Shokrpour, M.; Chamani, M.; Asemi, Z. The Effects of Magnesium-Zinc-Calcium-Vitamin D Co-Supplementation on Biomarkers of Inflammation, Oxidative Stress and Pregnancy Outcomes in Gestational Diabetes. BMC Pregnancy Childbirth 2019, 19, 107. [Google Scholar] [CrossRef]
- Jamilian, M.; Sabzevar, N.K.; Asemi, Z. The Effect of Magnesium and Vitamin E Co-Supplementation on Glycemic Control and Markers of Cardio-Metabolic Risk in Women with Polycystic Ovary Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Horm. Metab. Res. 2019, 51, 100–105. [Google Scholar]
- Nouri, K.; Walch, K.; Weghofer, A.; Imhof, M.; Egarter, C.; Ott, J. The Impact of a Standardized Oral Multinutrient Supplementation on Embryo Quality in in Vitro Fertilization/Intracytoplasmic Sperm Injection: A Prospective Randomized Trial. Gynecol. Obstet. Investig. 2017, 82, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Firouzabadi, R.D.; Aflatoonian, A.; Modarresi, S.; Sekhavat, L.; MohammadTaheri, S. Therapeutic Effects of Calcium & Vitamin D Supplementation in Women with PCOS. Complement. Ther. Clin. Pract. 2012, 18, 85–88. [Google Scholar] [PubMed]
- Rashidi, B.; Haghollahi, F.; Shariat, M.; Zayerii, F. The Effects of Calcium-Vitamin D and Metformin on Polycystic Ovary Syndrome: A Pilot Study. Taiwan J. Obstet. Gynecol. 2009, 48, 142–147. [Google Scholar] [CrossRef]
- Jaripur, M.; Ghasemi-Tehrani, H.; Askari, G.; Gholizadeh-Moghaddam, M.; Clark, C.C.T.; Rouhani, M.H. The Effects of Magnesium Supplementation on Abnormal Uterine Bleeding, Alopecia, Quality of Life, and Acne in Women with Polycystic Ovary Syndrome: A Randomized Clinical Trial. Reprod. Biol. Endocrinol. 2022, 20, 110. [Google Scholar] [CrossRef]
- Rayman, M.P.; Searle, E.; Kelly, L.; Johnsen, S.; Bodman-Smith, K.; Bath, S.C.; Mao, J.; Redman, C.W.G. Effect of Selenium on Markers of Risk of Pre-Eclampsia in UK Pregnant Women: A Randomised, Controlled Pilot Trial. Br. J. Nutr. 2014, 112, 99–111. [Google Scholar] [CrossRef]
- World Health Organization; FAO. Vitamin and Mineral Requirements in Human Nutrition; World Health Organization: Geneva, Switzerland, 2004; ISBN 9789241546126. [Google Scholar]
- Rayman, M.P. Selenium and Human Health. Lancet 2012, 379, 1256–1268. [Google Scholar] [CrossRef]
- Institute of Medicine (US). Committee to Review Dietary Reference Intakes for Vitamin D and Calcium. In Dietary Reference Intakes for Calcium and Vitamin D; Ross, A.C., Taylor, C.L., Yaktine, A.L., Del Valle, H.B., Eds.; National Academies Press (US): Washington, DC, USA, 2011. [Google Scholar]
- Hennigar, S.R.; Lieberman, H.R.; Fulgoni, V.L., 3rd; McClung, J.P. Serum Zinc Concentrations in the US Population Are Related to Sex, Age, and Time of Blood Draw but Not Dietary or Supplemental Zinc. J. Nutr. 2018, 148, 1341–1351. [Google Scholar] [CrossRef] [PubMed]
- DeLoughery, T.G. Iron Deficiency Anemia. Med. Clin. N. Am. 2017, 101, 319–332. [Google Scholar] [CrossRef]
- Catharine Ross, A. Modern Nutrition in Health and Disease; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2014; ISBN 978-1-60-547461-8. [Google Scholar]
- Institute of Medicine; Food and Nutrition Board; Standing Committee on the Scientific Evaluation of Dietary Reference Intakes. Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride; National Academies Press: Cambridge, MA, USA, 1999; ISBN 978-0-30-906403-3. [Google Scholar]
- Bo, S.; Durazzo, M.; Gambino, R.; Berutti, C.; Milanesio, N.; Caropreso, A.; Gentile, L.; Cassader, M.; Cavallo-Perin, P.; Pagano, G. Associations of Dietary and Serum Copper with Inflammation, Oxidative Stress, and Metabolic Variables in Adults. J. Nutr. 2008, 138, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Ambroziak, U.; Hybsier, S.; Shahnazaryan, U.; Krasnodębska-Kiljańska, M.; Rijntjes, E.; Bartoszewicz, Z.; Bednarczuk, T.; Schomburg, L. Severe Selenium Deficits in Pregnant Women Irrespective of Autoimmune Thyroid Disease in an Area with Marginal Selenium Intake. J. Trace Elem. Med. Biol. 2017, 44, 186–191. [Google Scholar] [CrossRef]
- Tulić, L.; Vidaković, S.; Tulić, I.; Ćurčić, M.; Bulat, Z. Toxic Metal and Trace Element Concentrations in Blood and Outcome of In Vitro Fertilization in Women. Biol. Trace Elem. Res. 2019, 188, 284–294. [Google Scholar] [CrossRef]
- Pitkin, R.M.; Gebhardt, M.P. Serum Calcium Concentrations in Human Pregnancy. Am. J. Obstet. Gynecol. 1977, 127, 775–778. [Google Scholar] [CrossRef] [PubMed]
- Polzikov, M.; Blinov, D.; Barakhoeva, Z.; Vovk, L.; Fetisova, Y.; Ovchinnikova, M.; Tischenko, M.; Zorina, I.; Yurasov, V.; Ushakova, T.; et al. Association of the Serum Folate and Total Calcium and Magnesium Levels Before Ovarian Stimulation With Outcomes of Fresh Fertilization Cycles in Normogonadotropic Women. Front. Endocrinol. 2022, 13, 732731. [Google Scholar] [CrossRef]
- Kurzel, R.B. Serum Magnesium Levels in Pregnancy and Preterm Labor. Am. J. Perinatol. 1991, 8, 119–127. [Google Scholar] [CrossRef]
- Pan, Z.; Cui, T.; Chen, W.; Gao, S.; Pearce, E.N.; Wang, W.; Chen, Y.; Guo, W.; Tan, L.; Shen, J.; et al. Serum Iodine Concentration in Pregnant Women and Its Association with Urinary Iodine Concentration and Thyroid Function. Clin. Endocrinol. 2019, 90, 711–718. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, K.G.; Andersson, M.; Hunziker, S.; Zimmermann, M.B.; Moore, S.E. Effects of an Iodine-Containing Prenatal Multiple Micronutrient on Maternal and Infant Iodine Status and Thyroid Function: A Randomized Trial in The Gambia. Thyroid 2020, 30, 1355–1365. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Minerals and their influence on hormonal regulation, ovarian function, and endometrium throughout the menstrual cycle. The graph (a) illustrates hormone fluctuations during the menstrual cycle, the sequence of images (b) depicts the progression of ovarian follicle development, and the illustration (c) shows the corresponding changes in the endometrium’s thickness. In subfigure a, the different colors represent the varying levels of specific hormones over the course of the menstrual cycle: black for GnRH, blue for estrogen, orange for progesterone, red for luteinizing hormone (LH), and green for follicle-stimulating hormone (FSH), each peaking at different times to regulate the cycle.
Figure 1.
Minerals and their influence on hormonal regulation, ovarian function, and endometrium throughout the menstrual cycle. The graph (a) illustrates hormone fluctuations during the menstrual cycle, the sequence of images (b) depicts the progression of ovarian follicle development, and the illustration (c) shows the corresponding changes in the endometrium’s thickness. In subfigure a, the different colors represent the varying levels of specific hormones over the course of the menstrual cycle: black for GnRH, blue for estrogen, orange for progesterone, red for luteinizing hormone (LH), and green for follicle-stimulating hormone (FSH), each peaking at different times to regulate the cycle.

Figure 2.
Oxidative Stress on the Uterus.

Table 2.
Recommended daily mineral intake for women and primary dietary source. This table provides a comprehensive overview of several key minerals that are important for fertility (Zn, Fe, Se, Ca, Mg, I, Cu, and Mn). For each mineral, the table lists the recommended daily intake, the actual intake levels used in various studies, the main food sources, and the optimal serum levels. In this document, ‘N.A.’ signifies ‘Not Available’, which is used to indicate that specific information or data sought in the context of the study could not be obtained or was not accessible at the time of the research.
Table 2.
Recommended daily mineral intake for women and primary dietary source. This table provides a comprehensive overview of several key minerals that are important for fertility (Zn, Fe, Se, Ca, Mg, I, Cu, and Mn). For each mineral, the table lists the recommended daily intake, the actual intake levels used in various studies, the main food sources, and the optimal serum levels. In this document, ‘N.A.’ signifies ‘Not Available’, which is used to indicate that specific information or data sought in the context of the study could not be obtained or was not accessible at the time of the research.
| Mineral | Zn | Fe | Se | Ca | Mg | I | Cu | Mn |
|---|---|---|---|---|---|---|---|---|
| Recommended daily intake | 8–11 mg [398] | 18–27 mg [399] | 55–60 µg [400] | 1000–1200 mg [401] | 320–350 mg [402] | 70–130 µg [403] | 1.3 mg [404] | 3 mg [405,406] |
| Daily intake in studies | 40 mg [407]–50 mg [72,408,409] | 60 mg [102] 100 mg [410]–250 mg [410,411] | 70 µg [412] | 1000 mg [413,414] | 250 mg [409,415] | 60 μg [416] | 1 mg [102] | 3 mg |
| Main food source | Meat, dairy, nuts, whole grains [405] | Leafy Greens, Meat, Legumes [417] | Brazil nuts, fish, whole-wheat bread [418] | Dairy products, fortified foods, leafy greens [419] | Green leafy vegetables, nuts, seeds, whole grains | Brazil nuts, fish, whole-wheat bread [418] | Oyster, nuts, sunflower seeds, liver, whole grain, dark chocolate | Brown rice, hazelnuts, chickpeas, spinach, pumpkin seeds |
| Recommended serum levels | 70–120 µg/dL [420] | 15–150 ng/mL [421] | 70–150 ng/mL [422] | 8.6–10.2 mg/dL [419] | 1.7–2.2 mg/dL [423] | 100 µg/L (Urine) | 70–150 µg/dL [424] | 4–15 µg/L [405] |
| Optimal serum levels in studies | ≥56 μg/dL [78] | N.A. | 45 μg/L [425]–109 μg/L [426] | 8.8–10.4 mg/dL [427] and <94 mg/L [428] | >1.4 mg/dL [429] 20.7 mg/L [428] 2.22–3.48 mg/dL [426] | 79.9–138.5 μg/L [430] and >150 μg/L (urinary) [431] | 88–177 μg/dL [405,426] | N.A. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kapper, C.; Oppelt, P.; Ganhör, C.; Gyunesh, A.A.; Arbeithuber, B.; Stelzl, P.; Rezk-Füreder, M. Minerals and the Menstrual Cycle: Impacts on Ovulation and Endometrial Health. Nutrients 2024, 16, 1008. https://doi.org/10.3390/nu16071008
AMA Style
Kapper C, Oppelt P, Ganhör C, Gyunesh AA, Arbeithuber B, Stelzl P, Rezk-Füreder M. Minerals and the Menstrual Cycle: Impacts on Ovulation and Endometrial Health. Nutrients. 2024; 16(7):1008. https://doi.org/10.3390/nu16071008
Chicago/Turabian StyleKapper, Celine, Peter Oppelt, Clara Ganhör, Ayberk Alp Gyunesh, Barbara Arbeithuber, Patrick Stelzl, and Marlene Rezk-Füreder. 2024. "Minerals and the Menstrual Cycle: Impacts on Ovulation and Endometrial Health" Nutrients 16, no. 7: 1008. https://doi.org/10.3390/nu16071008
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.